
New Zealand interlude
My family were quite surprised and disappointed when I announced that I had an appointment in New Zealand. I failed to tell them of the circumstances of my turning down the offered roster at the Royal Adelaide Hospital and the desperate plea which was apparent in the advertisement emanating from New Zealand.
I faced the prospect with mixed feelings. It would be a breath of fresh air after the claustrophobia of having to live at home for a six-year course, of seeing the same people every day during my course. It would be a huge challenge, the prospect of which left me more than a little apprehensive as I had not lived away from home before. But it was different and exciting. I would be thrown in at the deep end and have to fend for myself.
I booked my fare and was disappointed to find that the huge Sunderland Flying Boats that ran the regular route from Rose Bay in Sydney to Auckland Harbour had been withdrawn from service a few months before and had been replaced by standard four-engined Lockheeds.
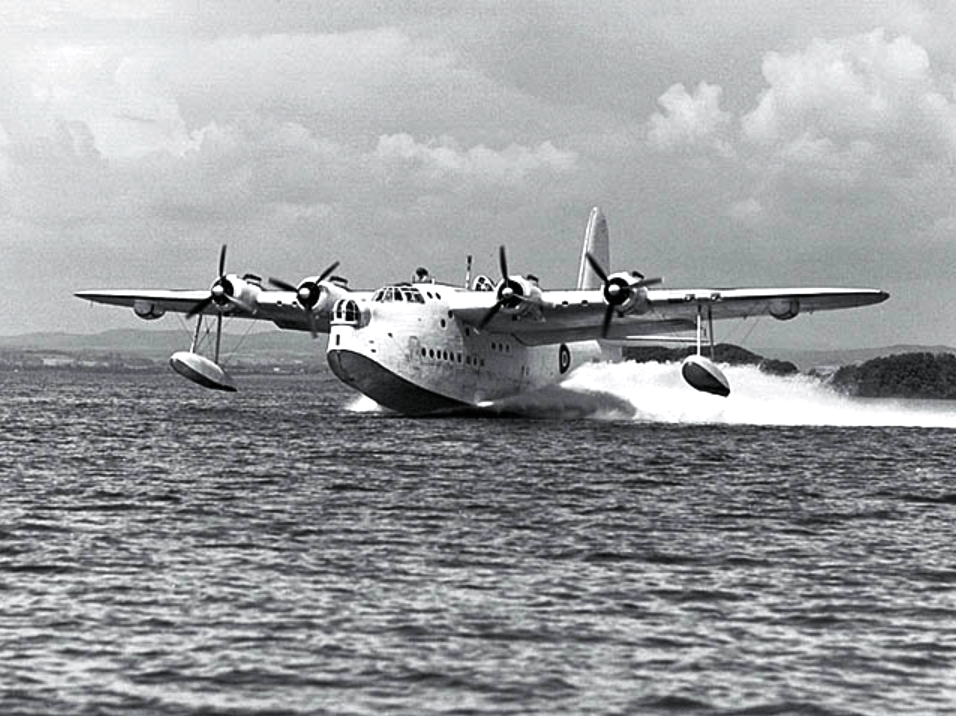
Sunderland Flying Boat
In May, 1958, I began my adventure. En route in Sydney, I had the pleasure of being best man at my good friend’s wedding – Bill Mann. The wedding went well and I therefore started off in good humour.
The flight to New Zealand landed in Christchurch and then a smaller plane transferred those passengers wanting the North Island to Wellington. Several, including myself, had destinations up the west coast, so we were transferred to an enormous stretch limo which meandered its way over a winding road to Whanganui, some two hour’s drive.
I was delivered to the front door of the Whanganui Hospital where the driver unpacked my luggage and departed to the next port of call. It was around 11.00pm and a night porter helped me into the residents’ quarters which were situated upstairs just inside the hospital entrance.

Whanganui Hospital around 1930
Imagine my surprise to find a party in full swing in the residents quarters. I was introduced all round to the well lubricated residents who were expecting me. I learned later that they had been told that they would be short staffed with three residents, instead of the normal four, for the rest of 1958, so my arrival was a cause for celebration. A couple of sixth year students from Dunedin were doing holiday locum house surgeon jobs at the time, so it was an excellent party. One of the sixth year students, Bruce Hamilton, had a fine baritone voice and, after giving us his rendition of Walzing Matilda, he launched into excerpts from Guys and Dolls which was the popular musical of the day. Everyone joined in and it was a raucous party; good party animals the New Zealanders, as I was to find out over the next year.
Well, if I was homesick when I arrived, it did not last long, and we all fell into bed about 3.00am. I felt at home amongst friendly colleagues, whom I knew would help me to acclimatise. The room I was allocated had a full view of the three North Island mountains, Ruapehu, Tongariro and the smoking Ngarahoe, their peaks covered in snow. It was all very exciting.

Present day Whanganui with Mt. Ruapehu, North Island’s highest peak, in the distance
I quickly became aware of the different arrangement of hospitals in New Zealand. There were large teaching hospitals in all the major cities like Auckland, Hamilton, Wellington, Christchurch and Dunedin but for the smaller centres like Whanganui, Masterton, Rotorua, Napier, Palmerston North, Timaru and a number of others, there were small hospitals of, say, 150 beds. They were served with specialists in Medicine, Surgery, Orthopaedics and Obstetrics but poorly provided for in the subspecialties of Eyes, ENT, etc. There were three qualified general surgeons, one of whom acted as hospital superintendent and was in charge of the hospital, plus two physicians, a tuberculosis physician (unqualified) and an obstetrician, together with two specialist anaesthetists. There were no resident registrars (specialists in training), just four resident house surgeons of whom I was one. We junior doctors ran the hospital. If we ran into trouble or were out of our depth, we called the appropriate consultant, each of whom, of course, ran their own small private practices and were paid on a sessional half day basis for working in the public hospital. There were several smaller private hospitals in Wanganui, none of which were geared for major conditions, so, in effect, there was little private practice in the town and any significant illnesses and accidents came to the public government-run hospital. My understanding was that there was no private health insurance in New Zealand at that time.
I also quickly became aware that New Zealand graduates were far better trained as practical doctors than their counterparts in Australia. During their medical course at Dunedin, the students, from fifth year onwards, were regularly rostered out to the provincial hospitals for practical experience and expected to take full responsibility under the visiting consultant. This included major decision-making for the patients who were admitted under their care.
If one elected to do Medicine during the period I was in New Zealand (1958-59), the only training available was at Dunedin, so medical students had to shift into lodgings there or, for a lucky few, live in a university college. In those days, Dunedin was a town which revolved around the university. It was founded by Scots, settled by Scots and run on frugal Scottish lines. Dunedin is Gaelic for Edinburgh. The discovery of gold in 1860 resulted in a huge boost to its population.
I found myself on a steep learning curve but, fortunately, my house surgeon colleagues were kind and patient teachers. House surgeons in New Zealand were expected to operate on all appendices, Colles fractures (broken wrists) and ankle fractures as well as performing curettes after miscarriages and dealing with the host of misadventures that found their way through the casualty doors. There was a radiographer present during office hours but after hours we took the films ourselves and developed them in hypo and fixer in the X-ray department. For the Colles fractures and ankle fractures we had a portable machine in the anaesthetic room where we did the reductions (manipulation and castings) under anaesthesia performed by one of our fellow house surgeons. We took our own post-reduction x-rays and took the plates around to the x-ray department where we developed them. In consultation with the house surgeon anaesthetist, we decided whether the reduction was adequate or not. If not, we did it all again until we were both satisfied. Well-padded plasters were applied and the patients were woken up and discharged to see the orthopaedic surgeon at his next outpatients.
Less than ideal treatment for sick patients, you might reasonably say. Yes, but great practical training for embryo doctors – and it came very cheaply for the NZ Health Service.
Of course this necessitated the house surgeons being competent at giving anaesthetics. My medical training in anaesthetics in Adelaide consisted of being accredited as having given ten rag and bottle ether anaesthetics under supervision to poor patients admitted after miscarriages to Da Costa Gynae Ward in the Adelaide Hospital.
These curettes were performed on a daily basis in a little theatre set up at the back of the ward and we were taught the rudiments of stages one, two and three of the anaesthetic levels. Of course, the patients had a terrible recovery with persistent vomiting but it was thought to be the safest technique to teach young doctors going into general practice.
It was far more sophisticated in New Zealand in 1958 where my fellow house surgeons expected intubation with an endotracheal tube for their appendix operating conditions. I quickly purchased a small book on anaesthetics and familiarised myself with the effects of the short-acting muscle paralyser Scoline and the slower but longer acting Tubarine. In no time, I was intubating patients without supervision and puffing the bag on the Boyles machine with nitrous oxide and oxygen. Scoline apnoea? Yes, we had the occasional case but I was fortunate and it did not occur with my patients. Oh, to be young and full of confidence in one’s ability.
I remember my greatest anaesthetic triumph occurred later in the year when I had an urgent call to theatre. A young Scottish graduate who had just joined us as a house surgeon was giving an anaesthetic for an appendix and the patient was having a horrible laryngeal spasm and had become very blue. It is said that a laryngeal spasm will relax before death ensues but I am not so sure. I took over the anaesthetic, put in some intravenous Scoline and put down an endotracheal tube and with a flourish said , “He’ll be OK now Mac, you just carry on and call me if you need me!” With that, I exited the theatre, brushing off his gratitude. “No worries,” I said.
The unmarried house surgeons lived in quarters above the main hospital block, with their own entrance up a winding staircase. We each had a bedroom and there was one community bathroom. We had a large sitting room and dining table with a big window looking out over the snow-covered peaks in the Tongariro National Park some 50 kilometres away. The married house surgeons had their own small units beyond the hospital grounds. At the time I arrived, there was only one unmarried house surgeon, John David de Villiers Taylor, and a couple of married house surgeons occupying the units. John was a big, brawny New Zealander in the mould of Edmund Hillary, with the same large jaw. We became very close friends and I attended his wedding in Wanganui later that year. I admired his competence and skill and he was very much my mentor in those early months.
John and I had all our meals together brought up from the kitchen by our personal maid, a middle-aged, motherly soul who cleaned the quarters, made our beds and took our washing to the hospital laundry. The meals were first class. The main meal was lunch and the table would be loaded down with usually two roasts and roast vegetables followed by sweets. John had an enormous appetite to match his size and would always pass his judgement on the quality of the meat.
My recollection of the breakfasts is of the Chinese gooseberries which I had never seen before and which later became known as Kiwi fruit. The evening meal was lighter but always tasty.
John set the rules, being the senior house surgeon. One of his rules was that if an ambulance came through the hospital gates one second after 6.00pm, then the patient it carried was the responsibility of the house surgeon on duty for the night. Many were the evenings that we would sit on the window ledge with our coffee, looking for an ambulance to come through those gates from the isolated Maori settlements of Pipiriki or Jerusalem, situated high up on the Wanganui River, and checking our watches to see whose responsibility the patient would be.
John became a very keen card player. He was not very good but enjoyed it immensely. I may have introduced him to pontoon, I don’t remember, but at every opportunity during our lunch hours he would get a team up into our quarters to play. There was no shortage of starters, Adrian de Frij, a Dutch physio, a lad from the biochemistry lab and one or two others. I would have preferred bridge but they all preferred a small gamble.
David Virtue was a house surgeon who lived with his wife in one of the married units. For some reason which I never discovered, he set up his record player, amplifiers and his great collection of classical records in our sitting room where they received plenty of use during recreational hours.
John and I had many happy times together and I was very sad to lose his company when he married and moved into one of the married quarters later in 1958. On one occasion, John arranged for the two of us to have a Friday evening drink after work at the Dominion, a pub patronised almost entirely by Maoris. We had a Maori friend who worked in one of the hospital laboratories but it was a major mistake to think we could match his alcohol intake. We found ourselves in a group of some eight or ten Maori blokes and the custom was that one would order a round of drinks – bloody Marys, Vodka and tomato juice – followed by the next in line ordering a chaser of Dominion bitter – a lethal combination with only one possible outcome. I looked in vain to see if there were any other pakehas in the hotel – there were none.
John and I staggered back to the hospital and took ourselves to bed. Sometime around 2.00am I awoke with violent cramps and nausea. The vomiting went on and on and, in desperation, I rang the night Matron, bless her, a very understanding soul. She fetched an injection of Stemetil, which she may have had to repeat. On the Saturday morning, I was due to front up on a ward round with Peter Powles, the senior physician of the hospital.
My term with Peter had started off rather poorly. We worked long, long hours in the hospital and, on one occasion, a number of medical cases had been admitted under his care. It was my job to document these cases – take their history and examine them and decide on a diagnosis. At midnight on this occasion, I had still not finished but I fell into bed, exhausted. The next day on his ward round, my inadequacy naturally came to light.
“Why haven’t you taken this case Johnson, that’s your job?” he started, and continued on in the same vein. I snapped and told him I had been up until midnight doing my best and if that was not good enough, he had better get himself another house surgeon. This took him aback more than somewhat and he paused to absorb my barrage. “Oh well, I’m sorry,’”he said finally, in a deflated tone and we moved on to the next patient.
On the morning after our big drink, I met up with Peter at 9.00am in the ward.
“You don’t look very well, Johnson,” he said to me after we seen a couple of patients. “Is something wrong?”
“Well sir,” I replied. “As a matter of fact, I think I may have picked up the ‘flu.”
“Well, best you take yourself back upstairs and go back to bed.” Never had I heard such welcome words.
After such a shaky start, Peter and I developed a good relationship. He even invited me to accompany him to a clinical meeting at Palmerston North. There, he talked briefly about his experiences with tuberculosis in the Maori population – a huge problem in Wanganui, which had a large population of Maoris living in villages and compounds up the Wanganui River.
When I left the hospital, Peter gave me an inscribed book, Adventures in New Zealand, which he had clearly chosen with care. I treasured it.

Taranaki, also known as Mt. Egmont, resembling Japan’s Mt. Fuji. It looks benign enough but whilst I was at Whanganui, twelve nurses were caught in a blizzard on its slopes and all perished.
In the fifties, it was fashionable for Adelaide medical graduates to travel to New Zealand to do their intern year. At the time I was there, we had Colin Bailey working at Masterton in the North Island. He came to spend a weekend with me at Wanganui. Later that year, he wrote to say he had had his appendix removed as a prerequisite to travelling to Antarctica to be the doctor at Mawson Base. I received a letter from him down there in which he waxed lyrically on racing across the ice behind his team of huskies. Colin finished up as a radiologist and, eventually, a radiotherapist at Hamilton in the North Island. He died quite young of prostate cancer.
Trevor Pickering was working at Ashburton and Ernie Urban was also at a provincial hospital, and at various stages I stayed with both of them.
Shortly after I arrived, a very raw intern, I was faced with a very difficult problem. I was called to casualty at about 8.00am to be confronted with a huge, muscle-bound man. He complained of having swallowed a chop bone which he felt was stuck in his throat. I was non-plussed by the situation and sought the help of my seniors. As I was due to assist at an operating list, I took him to the anaesthetic room where the specialist anaesthetist had a desultory look down his pharynx with his laryngoscope. Nothing to see, so I discharged him. Of course, the advice I should have been given would have been to contact the (unqualified) ENT doctor, who should have endoscoped him with our rigid oesophagoscope.
Low and behold, the man turned up back in casualty two days later with a rip roaring mediastinitis, an infection of the soft tissues around the oesophagus or gullet. Treatable perhaps in a big centre but in Wanganui in the fifties, it was a death sentence. He died two days later.
An inquest was held and, of course, the senior doctors threw me to the wolves, and I had to represent the hospital and give evidence. The coroner returned the finding that nothing could have been done to retrieve the situation and that the man, a Maori, had sustained a mortal injury. He should not have swallowed a bone! Nevertheless, his ghost walked across my roof for some years after.
What would one say in hindsight about the standard of care received by patients at Wanganui Hospital in the 1950s? The three general surgeons were of average competence. The conversation over the operating table was rugby union and who had played well the previous weekend and who didn’t. My impression was that they had a very restricted repertoire and occasionally attempted operations beyond their competence instead of referring them to a major centre.
One case that remains in my mind was a cancer of the stomach extending up into the oesophagus. The surgeon quickly became out of his depth, although he did the best he could and attempted suturing the remnant to the lower oesophagus. He then went on holidays, leaving the leaking anastomosis to a colleague who took no further action – and the patient died.
The operating theatre could be a caustic experience. On one occasion, I assisted the surgeon superintendant, John Trezise, who accused me of day-dreaming during a long operation: “Would you mind paying attention to what I am doing Johnson and take an intelligent interest!” In fact I enjoyed assisting and took such criticism poorly.
The shining light among the surgeons was the orthopaedic surgeon, Alan Cockerell, a young man well-trained and possessing an excellent pair of hands. The orthopaedic department under his direction was the best unit in the hospital.
The physicians were reasonably good. Peter Powles’s young assistant was a Richard Stone and he, like Cockerell, had recently arrived at the hospital as a consultant, was very up to date and keen to impart his knowledge on ward rounds. Even at that stage, however, I found the surgical attachments more to my liking.
The obstetrician was not allocated any resident staff. Often our general surgical list at 8.00am would start with a caesarean section.
The hospital possessed a large tuberculosis ward; TB was rife amongst the indigenous population in that era. The hospital also boasted a children’s ward and their medical or surgical problems came to our attention. I became quite adept at doing exchange transfusions for Rh incompatability and enjoyed the experience. I remember one poor little Maori child who had suffered extensive burns in a house fire and, over the course of three months, she needed multiple skin grafts. After being shown how to use the Humby knife these grafts were left to me and it gave me tremendous satisfaction to see a positive end result. I grew quite attached to this little uncomplaining girl over the period.
New Zealand is a beautiful country. In my mind, it has scenery equal to the best in the whole of Europe, all crowded into two small islands. On my weekends off, I went exploring. John Taylor’s father-in-law ran the Ford agency in Wanganui and had sold John a little Ford 10hp Prefect. John had the opportunity to upgrade to a newer model so I was able to purchase the old one at a good price. I flogged this little vehicle mercilessly around New Zealand, making the most of my time there. It never gave any trouble and I was able to sell it to someone in the hospital when I departed.
At the time I was in New Zealand, they were in the midst of a recession and luxury goods were difficult to come by. I had purchased a nice little Voigländer camera before leaving Australia as I knew it would be an essential item. John knew the pictures it could produce and was a keen buyer when I left, as they were unavailable in New Zealand. (This despite my having dropped it on the ice and cracked the viewing lens.)
One incident occurred which is worth relating, not in any way to demonstrate any smartness on my part, but because it gave me confidence and reinforced my determination to pursue a surgical career. I admitted to the surgical ward an acute abdomen under the care of the surgeon, Maurice Falloon, for whom I was working at the time. The woman clearly had severe clinical signs and I decided she needed an exploratory operation, and contacted Maurice who agreed with me and duly attended. As we were scrubbing up in theatre, he called on everyone to nominate their diagnosis. Three or four opinions were expressed and I nominated carcinoma of the ovary with secondaries and ascites (abdominal fluid collection). To the surprise of all present there it was – ovarian carcinoma with associated ascites.
“Congratulations Johnson, you’ve won the money!” announced Maurice. This did my confidence no end of good although, sadly for the patient, it was a death sentence.
Maurice was a kindly, quiet man and I enjoyed working for him. I remember that on Christmas Eve he donated and personally delivered a dozen bottles of Dominion Bitter to our upstairs quarters. As John Taylor and I were the only residents we thought it was a very generous gesture.
Without doubt, my sojourn in New Zealand confirmed that surgery was for me. Serendipitously, it transpired that New Zealand was the ideal spot to cut one’s teeth in this area of Medicine.
So sure was I that this was the direction in which I wished to proceed, I began studying for the Primary Exam of the College of Surgeons. I dug out my old Cunningham’s Dissecting Manuals which I had brought with me and attempted to make a start – but it turned out to be just a token gesture, as we worked long and heavy hours. I had a mammoth task was ahead of me, not having enamoured myself to the Adelaide hierarchy nor distinguishing myself academically. To enter the training program in surgery in Adelaide, one had to have achieved distinctions in exams during the medical course and/or have friends in high places. I fulfilled neither of these criteria – but hope springs eternal and I decided to take it step by step and see what happened.
Why would I want to embark on such an ambitious project anyway? I had a medical degree; surely that was enough? But the fire of ambition had been lit in New Zealand – and I was driven by the example of my father, who worked hard and long and pulled himself up by his bootstraps after leaving school at age thirteen. I think he had passed on the gene of unquenchable ambition, as well as, I regret to add, prostate cancer. But one must accept the bad with the good – and ‘one has to dance with whomsoever or whatsoever one brings to the dance’, as my best friend Des McDonnell was prone to say.
My colleagues at the hospital persuaded me that while I was in New Zealand, I should tackle the Milford Track – a three day walk in the south-west corner of the South Island, covering 53 kilometres and climbing up over the McKinnon Pass. With several companions, including a couple of lads from Sydney, I arranged some summer holidays and booked in. It was strenuous but great experience walking (or tramping as they say in NZ) through virgin bush and high country. I was fortunate to repeat the walk with my wife Sadie some 50 years later. It was equally spectacular – and I was even able to find my signature in the book kept at Milford Sound and entered some 50 years earlier.

The magnificent Mitre Peak at Milford Sound at the end if the Milford Track
In preparation for the trip, someone in the hospital had lent me a portable gas cooker. The week before leaving, I thought I should familiarise myself with its workings and proceeded to sort it out, of all the stupid places, in our sitting room situated in the main hospital block. On the carpet I filled the little open reservoir with methylated spirits, set it alight, and tried to pressure pump it. Suddenly, the whole caboose was in flames which quickly reached a height of about two metres, spreading onto the carpet. What to do? I had visions of a major fire and the whole hospital burning down and these were certainly realistic. I picked up the flaming burner and carried it down the stairs to the mezzanine floor which housed our bathroom and flung it into the bath and turned on the shower full bore. This doused that part of the fire whereupon I raced upstairs and with cushions put out the less-fiercely-burning fire on the carpet, then slumped into a sofa. There had been no-one else around. I surveyed the damage which was not too bad, all things considered. The carpet showed minor damaged and, when I inspected the bathroom, the worst damage seemed to be a huge black circle on the ceiling where the flames had licked but, fortuitously, not taken hold.
But I had second degree burns to both forearms. They were completely blistered and raw from the elbows to the palms. I thought it a reasonable outcome, having avoided burning the place down. About this time, John arrived on the scene and we both considered the next move. We chose not to report the incident, hoping no-one would notice the blackened ceiling in the bathroom, used only by us. John kindly summoned Sister Watts, who ran the theatre, and she and John dressed my burns with tulle gras and bandages. Again, I thought myself fortunate not have caused a major catastrophe and stymied any career plans.
I think I may already have been on holidays so, over the next few days, I quietly slipped out of the hospital gates en route to the Milford Track, stopping on the way at Masterton Hospital where my Adelaide colleague, Ernie Urban, redressed my wounds, and again at Ashburton Hospital, where my good friend Trevor Pickering was only too happy to do the same. Fortunately, on my return to duty at Wanganui Hospital, I was rotated on to a medical ward and was able to avoid scrubbing up in theatre which would have been impossible.
My twelve-month stint at Wanganui finished in May, 1959, by which time I was ready to return to Adelaide. I wrote to the Superintendent at the Adelaide Hospital, Bernard Nicholson, and was indeed fortunate that he bore me no grudge following on from my interview a year earlier when I had declined his job offer. On this occasion, he offered me an appointment as a senior house surgeon at the RAH – and this time I gratefully accepted.
When I went to the Lay Superintendant of the Wanganui Hospital to request my fare back to Australia, he denied any knowledge of such an offer ever having been made. Fortunately, I had kept the original advertisement and was able to present it to him. He quickly backed down but without any apology, and paid me my dues.
I had made many close friends at the hospital. We were a small group and mixed socially as well as during work hours. My last week there seemed like party after party – hectic, to say the least.
A final very sad epilogue to this New Zealand adventure occurred, which, over the intervening years, has upset me a great deal. My very close friend, John Taylor, with whom I spent many happy, laughing hours, married a delightful physiotherapist, Barbara, during the latter part of my stay. I caught up with them both at Auckland airport when I was en route to Canada to take up an anatomy teaching job some 18 months later. That was the last time I saw John who was embarking on a physicians training course. I heard indirectly that he had abandoned those plans and went into general practice at Taupo.
Over a number of decades I tried to locate John but without success. I even delegated one of my colleagues who was on an exchange to NZ to check with the New Zealand Medical Association, again without success.
Finally, after retiring, and on a trip to New Zealand around 2005, I pursued my search more aggressively with the New Zealand Medical Association and at last obtained a phone address at Blenheim in the South Island. Barbara answered the phone and to my absolute dismay informed me that John had died two weeks earlier after a long struggle with bowel cancer. I had been unable to locate them as they had spent many years in Riyadh, Saudi Arabia, where John was in charge of the Emergency Department. Barbara had returned to physiotherapy and was in charge of that department. When he was diagnosed with cancer, they had returned to New Zealand for treatment but the disease was beyond a cure. Barbara was running their small vineyard at Blenheim by herself.
I was devastated to miss John by a matter of weeks after all my attempts to find him. He was a friend, dear to me, and my affection was undiminished by the passage of the best part of 50 years. I had never given up hope of renewing that friendship. He was like the brother I never had, so close did we become in my twelve months at Whanganui.
READ Chapter 3
