
The Birth of Laparoscopic surgery
Laparoscopic surgery was first embraced in Adelaide by gynaecologists in the early seventies as being minimally invasive and it was certainly a major advance in minor procedures such as tubal ligation.
Some gynaecologists were more adventurous than others and I remember that in the early 1990s we had the odd divided ureter coming to TQEH as gynaecologists honed their skills in the development of laparoscopic hysterectomies at the Western Community Hospital.
One of those extending the frontiers at WCH was Robert Jones, now Rosie Jones, who in 2014 hit the news for different reasons, coming out as a transgender at the age of 67.

Dr Rosie Jones – image courtesy Australian Doctors news 5 November 2014
A fearless trailblazer was Jones. What courage it took to return to her old school, Prince Alfred College – a macho boys’ school, no less – and appear on stage in front of the entire school at the ‘Old, Old Boys Assembly’. gathering and mingle among the stooped, grey-haired old geriatrics, Rosie was replete with high heeled shoes and matching handbag – proudly and boldly standing and waving to all the boys as her name was called. After a brief second of stunned silence, the whole assembly erupted into wild applause and cheering. Joining in were all the present teaching staff and headmaster. Never before in the school’s illustrious 125-year history had anything like this occurred.
In 1985, the first laparoscopic cholecystectomy was performed by Erich Mühe in Germany and in the latter part of that decade it became clear that this was where surgery was heading.
In response, I attended numerous lectures and workshops, mainly interstate, to acquire the necessary skills.
I was approaching 60, perhaps a little late to be making major changes in my operative techniques. Colleagues of my vintage were rather hesitant and the more senior surgeons, John O’Brien and Bill Proudman, flatly refused to embrace these new techniques. Certainly, the learning curve was flatter than it had been 30 years earlier and it took some 18 months before I felt completely comfortable in this new approach to surgery.
Sometime in 1988-9, I performed the first laparoscopic cholecystectomy at TQEH on the public list. I chose what I thought would be an easy case – a slender girl of about 60 kilograms. However, as I later realised, excessively small patients are as difficult as those overweight. Nevertheless, it went well.
A short time later, I operated on the first laparoscopic cholecystectomy at the Western Community Hospital. This was a private patient, the first on my regular Wednesday list. What I hadn’t taken into account was that on Wednesday mornings, the hospital scheduled backup generator testing. Low and behold, at a delicate stage of the procedure, the monitor went blank. No electricity and no vision. It took some 20 minutes for it to reconnect but fortunately no harm was done.
Position of ports and setup for laparoscopic cholecystectomy


The early 1990s saw changes at TQEH. Bill Proudman retired and it was decided by the University Department of Surgery that, instead of three general surgical units, we would have three specialist units, in keeping with specialisation within surgery.
The Professorial Unit, headed by Professor Guy Maddern, chose the sub-specialty of Upper Gastrointestinal, including liver, pancreas and gall bladders as their area of expertise. The other two specialties that were decided upon were Breast Endocrine and Colorectal – and the remaining six Visiting Surgeons outside the University Department could toss a coin to decide where they would go. There was one proviso and that was that the Colorectal Unit would take Bill Roediger from the Professorial Unit.
Well, the rest of us tossed it about amongst ourselves and eventually agreed that Colin Paull and I would join Bill Roediger on a Colorectal Unit on the fifth floor and Trevor Pickering, Vlad Humeniuk and Rob Parkyn would form the Breast Endocrine Unit on the fourth floor.
In the Colorectal group, Colin Paull was the most senior but, as he also was close to retirement, he magnanimously nominated me to be Head of Unit. It was unexpected but also exciting as I had definite views on which way the unit should head, with laparoscopic techniques emerging. Colin possibly realised this in making his decision.
At the time, Queenslander Russell Stitz was probably at the forefront of laparoscopic surgery in Australia, with Sydney’s Professor Les Bokay just behind. Melbourne and Perth were not showing much enthusiasm. In Adelaide, the RAH was disinterested and TQEH was yet to get started.
Colin Paull, as mentioned, was on the point of retiring and was not keen to embrace new technology and Bill Roediger tended to go his own way, which left me and our enthusiastic Senior Registrar, Alex Karatassas, to further explore laparoscopic techniques. Alex was showing very good skills and was the right age to tackle new concepts. Our Professor, Guy Maddern, was encouraging.
Colin Paull (front left) at his retirement function with Peter Hewitt and Guy Maddern (front) and author with Tony Slavotinek standing
Bill Roediger had come to TQEH Department of Surgery from the Alfred Hospital in Melbourne. He was South African by birth and was well-qualified with MSc,PhD (Oxon), FRACS, and was appointed an Associate Professor. He solicited Colin Paull and me to follow his lead in doing low anterior resections for carcinoma with the anastomosis outside the rectum. He did three cases that I can recall and he enthusiastically described them to Colin Paull and me, although we never saw these cases on the ward. We didn’t pursue the procedure and Bill was not involved in our laparoscopic ventures.
Bill was a very good lecturer and had done work on inflammatory bowel disease and I was given to understand that he was internationally recognised for his research in this area. It would seem his forte was in the laboratory and research rather than the operating theatre but he confessed that he loved operating and so there was somewhat of an impasse. Bill went his way and the rest of us our way.

Alex Karatassas
We were lucky to have Alex Karatassas join us on the unit in 1992 with his background in pioneering laparoscopic procedures at Modbury Hospital with Mr Greg Otto. He was young, became increasingly confident in his ability, and took to laparoscopic bowel resections like a duck to water. I found him easy to work with and so he did most of our Monday afternoon operating assisted by me. I considered my role at the age of 60 to be a facilitator rather than primary hands on and so together we made a good team.
I have remained close friends with Alex in the 30 or so years since we worked together and have valued his repeated invitations for me to attend his seminars, which has given me continuing contact with colleagues. He remains at the forefront of technological advances and now leads a team in robotic surgery at Ashford Hospital.
In keeping with our determination to go down the laparoscopic path we commenced regular workshops in various animal houses. Initially, we used the IMVS Animal House and then moved to using the Animal House at TQEH, with financial and instrument help coming from pharmaceuticaul company Johnson & Johnson. They might have seen us as a long term investment but, nevertheless, we were grateful.
We had reasonable cooperation from the theatre staff. They, too, had to become familiar with very new techniques. I have already alluded to having the Johnson & Johnson reps in theatre which was strongly resisted. Having our own dedicated nursing sister every Monday afternoon was also strongly resisted but eventually agreed to. The hierarchy felt that the scrub sisters should be rotated every Monday so that they would all get the experience. We were keen to have few distractions while we were on such a steep learning curve and so managed to keep a dedicated scrub sister, at least in those early days.
The Colorectal Unit of The Queen Elizabeth Hospital commenced activity in January, 1990. We were staffed by three consultants, one senior and one junior registrar and had our own ward. The Unit had four operating sessions each week, together with two outpatient sessions, and participated in regular xray review sessions and pathology teaching commitments attended by the whole unit, including attached students in rotation.
In the early years of these specialised units, the work remained fairly general, as it had been agreed that specialisation would take place by evolution rather than by decree.
I attended all the Australian laparoscopic colorectal workshops advertised during 1991 and ’92 and then stumbled upon an annual workshop run by probably the best exponent of laparoscopic colorectal surgery in the world at the time, Morris Franklin, from San Antonio, Texas.
His second workshop was to be held in November, 1992, in Maui, Hawaii. From memory, I think he had earlier attended a workshop in Australia organised by Russell Stitz on Hamilton Island, which I also attended .
The hotel was well set up for conferences with a huge lecture auditorium and, in typical American style, the day kicked off at 6.30am and continued until 6.00pm, with lectures and demonstrations.
So, come November, 1992, Sadie and I packed our bags and were off to the Hyatt Regency Hotel, Maui. We were pleased to find Marx Wald and his wife Di were also at the conference. Marx was head of the colorectal unit at Royal Perth and they were both well known to us.
The highlight, I thought, was the practical session on pigs. The whole basement of the hotel was converted into an animal laboratory with probably some 50 pigs being anaesthetised and, in pairs and under instruction, we performed laparoscopic bowel resections to the best of our ability. The area was secured against animal liberationists and we were required to abide by strict protocols.
Dr. Franklin ran the show with charm and panache, introducing every speaker as, “Mah very good friend…” in his Texan drawl.
On the last day, we had a farewell BBQ around the hotel pool and I introduced myself to Morris. He was most gracious and friendly. I explained to him where we were in our learning curve and invited
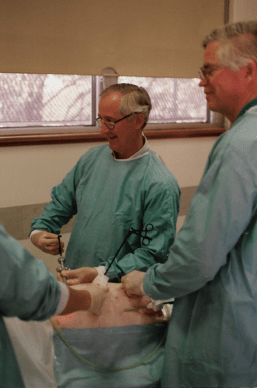
Author performing a bowel resection on a pig in the basement of the Regency Resort, Maui, assisted by Doug Handley from Adelaide
him to to visit us Without any hesitation he responded, “Well, of course ah’d come down to help you. Ah love Awstralia and would be only too happy to pay a visit.” What a nice man, I thought.
As well as being delighted with his response, I felt it to be a signature moment in the evolution of TQEH Colorectal Unit.
On return to Adelaide we set about planning his visit to our department with gusto.
TQEH had approved a dedicated operating theatre for our use every Monday afternoon. It was a major coup getting Theatre 8, a recently-added spacious theatre which gave us ample room for all the equipment and personnel associated with laparoscopic colorectal surgery.
For more than 20 years, my Monday afternoon list had been in Theatre 3, a poky little space with hardly any room to swing a cat. It was a double theatre, sharing a common entrance and phone with Theatre 1, where our Visiting Neurosurgeon, Harold Schaeffer, operated. The sudden ringing of this phone always startled Harold, to the extent that his forearms and neck would visibly spasm. If he were delicately dissecting in one of the hemispheres, a million or two neurones could bite the dust! It was eventually decreed that on Monday afternoons the phone would be disconnected and any messages would be delivered by the scout nurse.

Associate Professor Margaret Davey AM
Across the corridor on those Monday afternoons, Marg Davey AM would be operating in Theatre 4. She was a renowned oncological gynae surgeon who had spent 10 years training at the Norwegian Radium Hospital in Oslo. The cases presented to Marg were all cancer patients, either ovarian or uterine of one type or another. They were often at the margin of being operable or inoperable and of course the adjacent bowel was often involved. Many were the Monday afternoons that her registrar would wander across the intervening corridor to where I was operating: “Dr Davey wonders if you would mind popping across to theatre four?”
Our Monday afternoons were a movable feast – sometimes the registrar would perform the operation and I would assist or even leave him to it and be available in the tea room if he got into trouble. That was the way surgery was taught to registrars – one can only grow in confidence by doing it one’s self.
We were pleased to be allocated Theatre 8 – even more so when we managed to procure dedicated theatre staff for our laparoscopic procedures together with instruments donated by the Ethicon company. We had been concerned about the cost of these expensive instruments. and knew that as soon as the procedures were established in the hospital there would be no more freebees!
Alex Karatassas and I battled on together and made slow but steady progress up the learning curve.
Our first laparoscopic colorectal operation at TQEH was performed successfully in November, 1992 – a laparoscopic Ripstein repair. This was performed by Alex Karatassas assisted by me.
A few months later, we brought Russell Stitz down from Brisbane to demonstrate some techniques and, on another occasion, Tim Wilson from Sydney.

Russall Stitz demonstrating a laparoscopic procedurer using his button technique with Alex Karatassas and Nick Marshall assisting
Demonstrating his ‘button’ technique for repair of a prolapsing rectum, Russell lost the plot a little when one of his buttons which he used to attach the offending rectum to the sacrum jumped out of his instrument onto the floor, requiring resterilisation. He did not appreciate the mirth this created from the viewing audience! Two more tacks then fractured during insertion.
In 1993, Alex Karatassas embarked on a world tour visiting centres of laparoscopic excellence in the UK and United States, having been awarded a travel grant by The Queen Elizabeth Hospital. The tour included a couple of weeks with Morris Franklin in San Antonio, Texas, during which time Alex established a warm, close and lasting relationship with the professor, probably the world’s leading exponent of laparoscopic colorectal surgery at the time. The results of this trip proved to be extremely beneficial to the unit.
Alex, in fact, established such a rapport with Morris Franklin that he was invited to speak at his funeral by international video hookup in the middle of the night (Adelaide time), after he sadly died in 2020.
In April, 1993, Tim Wilson from the Sydney Hospital Endosurgical Unit spent two days with us lecturing and demonstrating laparoscopic procedures, performing on this occasion a laparoscopic anterior resection.
In that year, fourteen laparoscopic large bowel procedures were performed, predominately anterior resections, but also including several Ripstein repairs, a right hemicolectomy and an abdominoperineal resection.
In October 1994, Colin Paull turned 65 and reluctantly retired from TQEH – reluctantly, because surgery was the heart and soul of his life. He loved and lived for surgery. From the opening of the hospital in 1958 – when he was the first of two junior registrars with Tony Rieger on the Professorial Unit, both under Bill Proudman as Senior Registrar – Colin demonstrated his skills and experience as a colorectal surgeon. He soon became an Honorary Surgeon and throughout his 36 years at the hospital he was the principal colorectal surgeon, an area in which he set high standards.
Colins’ successor, appointed to the colorectal unit, was Peter Hewitt who had been earmarked for the appointment for some years.

Footnote: The author is forever grateful to Peter Hewett for saving his life in 2016 with an emergency ileostomy.
Peter had learned his trade as a colorectal surgeon with Russell Stitz in Brisbane, the foremost laparoscopic surgeon in Australia at the time. It is my understanding that Russell was desirous of having Peter join him in Brisbane but as Mary, his wife, was an Adelaide girl, and both families were from Adelaide, he declined and accepted our offer.
Peter had earlier been at TQEH as a senior registrar and his skills were well known to us. I consider Peter’s appointment was a coupe as I do not think our fledgling unit was itself of sufficient merit to attract him.
I think it was at this time that we decided that all future appointments to the unit would need be, like Peter, accredited by the Colorectal Society of Australia.
I had previously solicited James Moore and Richard Sarre to join our unit but both were too well established elsewhere to accept.
Throughout 1994, preparations were being made for a major Colorectal Seminar organised by the Colorectal Unit and this took place on Friday, March 10, 1995, with the drug firm Johnson & Johnson picking up the cost of bringing and accommodating Morris Franklin from Texas, along with Victor Fazio, Head of Colo-Rectal Surgery from the Cleveland Clinic, and Russell Stitz, President of the Australasian College, from Brisbane. The meeting had an excellent turnout with 120 registrants from around Australia and South East Asia and was well received. Morris stayed on to operate for a day or so after, and we got to know him better.

Morris Franklin, Victor Fazio and Russell Stitz
Morris’s arrival in Adelaide was a mini disaster. Sadie and I went to the airport to meet him and his wife. However, no wife – she had already caught a taxi to the casino where she spent most of his visit gambling. So much for the program Sadie had arranged for her! She didn’t accompany Morris on his subsequent trip.
I took Morris out to the Medical Board offices on Payneham Road, St Peters, to register his visit. There we were greeted by the secretary, with whom I’d had previous dealings.
“Hmm,” the secretary said with a smirk. “I see he only has a visitor’s visa, so he cannot do any operating.”
The secretary knew very well that operations had been arranged. I protested strongly but to no avail – and we were already running late for Morris’s first presentation.
At this stage, Morris intervened and said, “Leave this to me. Ah’ve had a coronary stent recently and resolved not to let any circumstance upset me.” He could see I was getting hot under the collar.
Turning to the secretary, he asked, “Now, mah good man, what do we have to do to change mah visa?”
“Well,” replied the secretary, seemingly enjoying himself. “You have to go into the city to Grenfell Street to the Immigration Department, join the queue and ask them to change your visitor’s visa to a working visa.” He omitted the obvious: ‘And find a parking spot!’….
Time was marching on and I was none too happy – but Morris clearly wanted the matter settled amicably. Then, as we stepped onto the footpath, Morris’s bag flew open and a myriad of pens and pencils and erasers and notes scattered all over the footpath. It was starting to look like a Peter Sellers’ comedy farce.
We retrieved the situation and drove to Grenfell Street where we fortunately found the nicest girl behind the counter. She quickly changed the visa and we returned to the Medical Board, where I stood back while Morris registered himself. And, finally, we were on our way to TQEH.
The meeting went well, as did the conference dinner. The final day of Morris’s visit was to be devoted to operating, with him demonstrating his technique in laparoscopic bowel resection. It did not start well. The first patient had accidentally been given a hearty breakfast and so was cancelled.
The second scheduled case, in retrospect, was an inoperable cancer of the upper rectum. Morris soldiered on with increasing amounts of blood being lost from the presacral veins. Our Professor, Guy Maddern, and I watched with the other spectators then slipped out to the corridor.
“Go in and tell him to stop and convert it to an AP resection!” demanded Guy.
“Go and tell him yourself, you’re the Professor,” I rudely retorted. So nothing happened and the anaesthetists continued to struggle with the increasing blood loss.
Eventually, Morris capitulated and his assistant, Peter Hewett, went down to the lower end and they converted the operation to an abdomino-perineal resection.
This procedure took an hour or so longer than expected and we all then adjourned to the tea room. The patient recovered from the operation but died a month or two later.
“Let’s cancel the last case Morris,” we suggested, as he was running late for a presentation at Flinders Medical Centre.
“Naw,” responded Morris. “Ah promised that lady that Ah would do her operation and Ah intend to keep that promise.”
And so the last case went ahead and, fortunately, Morris was able to demonstrate his superb skills and it was done in record time.
As mentioned earlier, our experiences that morning made us decide that fly in, fly out operating was not in the patients’ nor the surgeon’s best interests – and this was the last such operation performed by a visiting surgeon at TQEH.
One of our rest and recreation activities planned for that week was a golf game at Royal Adelaide Golf course. This was kindly arranged by Guy Maddern, a member of that club. I played with Guy’s father John, a passionate, single-figure handicap golfer who regularly scored less than his age, and Guy played with Morris.
A golf game teaches one a lot about one’s opponents and partners. Morris, I thought, probably only played about once a year, whilst the rest of us played regularly.
As it turned out, Morris played golf like he lived the rest of his life, and was not one bit embarrassed by spending a lot of time with his backside up in the bushes looking for his ball. He said that he enjoyed it and I certainly enjoyed partnering John, who had known my wife, Sadie, as a nursing sister at the Memorial Hospital when Guy was a baby. Adelaide is a small town.
Two of our surgeons, Alex Karatassis, and Peter Hewett subsequently went to San Antonio in Texas to work with Morris, each for a week or two, and this was of great benefit to our unit.
Perhaps they also learned a thing or two there about managing a relationship. After a hard day’s operating, it was Morris’s custom to go to his workshop and spend a couple of hours on his hobby – restoring vintage Rolls Royces! Home life, it would seem, played a very small role in his big scheme of things.
Morris returned to Adelaide again in 2013 for a further meeting and also in 2015. On each occasion, he was to box up and transport his 1923 open Rolls Royce tourer which he had lovingly restored, and drive it around Tasmania or along The Great Ocean Road in Victoria. In fact, on his last visit he considered purchasing a similar vintage Rolls Royce in Adelaide, to be available for subsequent visits.

A Rolls identical to that belonging to Morris
In 2015, Morris Franklin was in his early 70s, had had coronary artery stents around 15 years earlier and a bypass more recently.
“Are you planning to retire Morris?” he was asked.
“Ah plan to die with mah boots on in the operatin’ theatre – yes sir!”
On the first occasion we encountered Morris in 1995, he had brought with him his wife but, as mentioned earlier, she spent her whole time in Adelaide at the casino. On the last occasion, in 2015, he had with him a new partner, Carla Stone, and they spent some time patting and stroking each other on the social outings. Soon after, we received an invitation to ‘a Gala event under the Big Sky in Montana,’ a reference to a ranch he was building ‘overlooking the glorious Madison Valley’. The event would be ‘a Celebration of Life, of Friends, and Fellowship’ to be held on the property from August 6 – 9, 2015.
The closest airport? Fifty two miles away in Bozeman, Montana. Tempting as the invitation was, Sadie and I decided we were too old to face such a trip – but our good friends Alex Karatassas and partner Nita did pay him a visit.
Well, they say Texans are larger than life and most certainly this applies to Morris Franklin. A superb surgeon of vast experience with beautiful soft hands in the theatre. A great teacher and a towering world figure in surgery, generous to a fault – and it has been my good fortune to call him a friend.

Morris Emory Franklin 1942 – 2020
It would be remiss of me not to mention the tremendous support we had from Johnson & Johnson Australia during those early years. They regularly set up Saturday morning workshops, supplying all the instruments and teaching material for all of us on the unit to practice techniques. The reps (all women) used to also bring fresh scones and cream for morning tea. I particularly remember Karen Brown, who later gained her helicopter pilot’s licence and spent some time in the Northern Territory rounding up cattle by air! Some years later I came across her on the beach at Glenelg with a surf ski and dog which accompanied her on the ski riding the waves. Her partner, Clinton Habib, was a very talented artist. (And still is. Ed.)
We did have a bit of trouble with the Head Nurse, Sister Barbara Osborn-White, who initially argued against allowing the reps into theatre but the battle was won when it became clear their presence was invaluable – not only in providing a whole range of instruments but also in providing advice as to their best use. They were all well-trained in the use of these new tools and, ironically, were also of immense help in guiding the scrub sister.

Large bowel resection in progress at TQEH. From left Bill Roediger, author, Russell Stitz operating
Sister Osborne-White and I did not always see eye to eye for one reason or another. I remember whinging to Bob Magarey and he, with his long military experience, replied, “Ross, she’s army trained and when the Colonel comes around to do his weekly check on a Monday morning and says to her, ‘Sister, those sluices have not been cleaned’, her reply without hesitation would be, ‘They’re always cleaned on a Tuesday, Sir!’ “
I have had cause to reflect on my dealings with O-W in recent times. At one of our yearly reunion dinners at Kooyonga Golf Club in 2020, I met three former theatre sisters from TQEH.
One of them volunteered: “I complained about you to Sister Osborne-White after I thought you treated me harshly in theatre. She was unsympathetic to my complaint and told me you were really quite nice and declined to do anything.”
Well, some gentle admonishment never hurts anyone!
At one stage in about 1970, Bill Proudman decided to start a ‘Theatre Investment Club’ with Barbara Osborne-White as Executive Secretary. Each member would contribute a fixed amount each month and there would be regular meetings to decide on investments.
There was some excitement around the sharemarket at this time. The Adelaide owner of Poseiden No Liability, Norm Shierlaw, ignited a frenzy when shares in his stocks went from $1.00 to $280.00 in just six months. In early 1970, the bubble burst and a lot of people lost a lot of money.
One would have to say TQEH Investment Club was a failure. It continued for a couple of years before being wound it up. It did not lose money but nor did it make any.
Like a lot of other people, I dabbled a little at that time. For the first time in my life, I had a dollar in my pocket and it burnt a hole. I remember buying odd shares like ‘Flinders North’, but they all lost money in the subsequent correction and I departed the share market scene not returning until nearly three decades later – a much wiser man.
In that seventies era, surgeons, anaesthetists and other medicos were cannon fodder for unscrupulous borrowers. Surgeons and anaesthetists are great gossipers. The surgeon goes into cruise control as he operates and chats with his anaesthetist. They might dream up schemes for making money, urging each other on. One group of surgeons and anaesthetists decided a good scheme would be to buy a crayfish boat! It cost them a lot of money and they lost a lot of money. Another group of radiologists decided to invest in a cargo plane. It crashed, literally, and that enterprise also turned out to be very expensive.
The temptation in those days of very high taxes, including provision tax paid in advance of forecast earnings, was to find a way to minimise the tax burden. Unworldy medicos were sitting ducks for any crooked entrepreneur.
My private anaesthetist, Bill Mann, whom I used regularly for my private lists for 30 years, and whom I regarded as the best anaesthetist in town, was also surprisingly caught out in a small way in one of these schemes – investing in blackberry farms. It turned out to be a scam.
The person whom we employed to build our rooms in Walter Street, North Adelaide, took Trevor Pickering and myself for a ride. Although we could not fault him in the development of our rooms, he approached us later to invest in a pine plantation, Percheron, just out of Canberra. We made regular payments over several years amounting to many thousands of dollars but when it came to the thinning of the plantation after 15 years, it became apparent that it had been neglected, and no payments were forthcoming. It was a big organisation and subsequently became the subject of a class action but the lolly had long since gone.
It was a good lesson. What appears too good to be true is rarely good or true. Our developer left town in a hurry, eloping to South America with a radiographer from another group of medical rooms. There he resided for many years, perhaps ten, only returning when things weren’t so hot. He had the temerity to look up Trevor Pickering and me for more work. We politely brushed him off.
In December, 1994, I reached the age of 60 and decided to retire as Head of Unit. My place was taken by Bill Roediger, one of the three inaugural appointees to the Colorectal Unit.
At this time, commensurate with the increase in activity of the Unit, funds were made available by Guy Maddern to appoint an additional dedicated Colorectal Surgeon for three sessions per week. This appointment was offered to Jim Young, who commenced on the Unit in January 1997. Jim subsequently started a colorectal service at the Lyell McEwin as an outreach of our QEH service..
In 1997 TQEH and the Lyell McEwin Hospital amalgamated and shared a common Board of Management. The Lyell McEwin had not offered a specialised colorectal service at that time but provided general surgical services as we had at TQEH prior to 1990. As mentioned above TQEH commenced a skeleton Colorectal Service offering limited outpatient and operative services to the Lyall McEwin Hospital under the supervision of Jim Young.
The Unit was fortunate to have as our Senior Registrar at that time Chris Hensman, who had spent twelve months with Professor Alfred Cuschieri in Dundee, Scotland, participating in the running of his regular laparoscopic skills workshops.
Chris Hensman
During 1997, Chris and Alex Karatassas ran a fortnightly benchtop laparoscopic skills laboratory alternating with an Animal House operative procedure. These workshops were sponsored by Johnson & Johnson and proved a valuable avenue for the introduction of new instruments and new techniques into our laparoscopic large bowel procedures.
Peter Hewett also commenced an incontinence clinic in 1997 as he was interested in manometric studies and the stimulated graciloplasty procedure. It was planned to expand this weekly session with the addition of ancillary staff such as a physiotherapist and stomal therapist.
In 1997, the Colorectal Unit commenced a PR Bleeding Clinic in an area within the Day Surgery Unit to enable referring General Practitioners to make direct referrals, rather than having their patients go through the Outpatient Department. At this clinic, a history was taken, then physical examination and, where indicated, a flexible sigmoidoscopy and banding of haemorrhoids was carried out as a ‘one stop shop’, saving patients from making multiple outpatient appointments.
Another 1997 startup was genetic counselling, in coordination with Dr Graeme Suthers, who was at that time Chairman of the Familial Cancer Research Group and based at the Women’s and Children’s Hospital. The eventual aim was to be part of a multi-centre study.
The Colorectal Unit also had brief contact with Graeme Young when he joined TQEH as Professor of Medicine in 1995, his main interest being in the epidemiology, prevention and molecular biology of colorectal cancer. His stay at TQEH was shortlived, however, as he left to further his career at Flinders University.
It was a time of exploration and development. I made an approach to Wayne Singh, the CEO of Western Hospital at this time, to explore projects that might be mutally advantageous. I had a good relationship with Wayne as I operated regularly at his hospital and served as the College representative on his Medical Advisory Board.
My responsibility in that role was to monitor the standard of surgery performed there. Over the years we only had one occasion in which we were forced to suspend the operating rights of a surgeon.
Wayne expressed an interest in making space available and providing nursing assistance in the private section of the hospital as well as also offering treatment to public, non-insured patients. We discussed the possibility of our unit offering a regular, say twice weekly, flexible sigmoidoscopy service for PR bleeding patients, both public and private. Unfortunately nothing materialised from these discussions which could have developrd an interewsting melding of private and public hoepitals..
One hurdle ahead of us was to have the Colorectal Unit accredited by the Colorectal Society of Australia. The Guidelines circulated by the President of the Colorectal Surgical Society of Australia (September, 1996, Graham Newstead) specified that the surgical staff of such a unit should include two accredited colorectal surgeons, one of whom would be Head of Unit. When Jim Young joined us and Peter Hewett took over as Head of Unit all of these criteria were fulfilled and the unit, thereby, was accredited.
It would be fair to say our that in 1998 our unit came of age, having achieved national recognition, becoming accredted as a post-fellowship training centre for colorectal surgery, with the first post-fellowship trainee due to start the following year, in 1999.
