
Private surgical practice
In 1968, surgeons operating at private hospitals were expected to bring their own tools. They’d select those required for the particular procedure from their tool bags to be sterilised by the theatre staff. Clearly, buying new tools would be very expensive and I managed to get a well-used set on the second-hand market from a retiring surgeon.


Surgeons’ well used instrument bags from 1968
In fact, at the time I started out, a number of hospitals were finding that if they purchased their own instruments it was much more economical and gave them better control over the happenings in the operating theatre. Thus, over the next two or three years after I started in private pratice, my bag of instruments became redundant.
My first faithful referring GP in 1968 was Ian Murdoch, who had purchased the Karoonda practice after he left the employ of TQEH. Karoonda is in the SA Mallee area, very arid, and populated by tough citizens.
Ian invited me to do a regular monthly operating list at Karoonda with him giving the anaesthetics. Ian had learned his anaesthetics in the department at TQEH and I knew he was competent and safe. Our lists comprised fairly simple procedures like tonsils and adenoids, haemorrhoids, varicose veins, the odd grumbling appendix and various lumps and bumps, and we managed well. Having a visiting surgeon boosted his practice in the area and he later invited Frank Welch, a gynaecologist, to fill a similar role. The so-called hospital in those early days was an old house, with the various rooms divided into two and three-bed wards. The dining room was the operating theatre.
A few years after we started this surgical service, the government of the day, in their wisdom, decided to build a new state of the art hospital, with, not one, but two theatre operating suites. I don’t remember the cost but it was a very extravagant exercise, especially as Ian left Karoonda after ten years or so and his successors did not give anaesthetics and so dispensed with my operating. The two theatres to my knowledge were not ever utilised thereafter. It was far and away the grandest hospital building in the SA Mallee – a memoriam to the politicians, with no consideration given to the actual requirements of the local community or discussion with the medical providers.

The new Karoonda Hospital 1973
The opening I do remember, in about 1973. It was a large function and a political exercise in self-aggrandisement with not one word mentioned of Ian Murdoch nor the visiting specialists.
Ian built up a strong following around the Mallee and we used to get patients from, Wynarka, Borrika, Sandalwood, Perponda, Copeville, Bow Hill, Kalyan, Halidon, Sherlock, Buccleuch, Galga, and as far away as Peake and Nildottie on the river. We even saw the odd patient from Tailem Bend and occasionally Murray Bridge who had become disgruntled with these larger practices.

Karoonda patient drainage area
On occasions, Ian would ring late of an evening to tell me he had an appendix which required operation. I would always hope he’d say, ‘Can you find a bed in Adelaide and I will send the appendix down’ – but he never did. And so I would climb into my trusty old secondhand Falcon station wagon and flog it up the old Murray Bridge Road – no freeway in those days. The road wound through Hahndorf, Mount Barker, Kanmantoo and then followed the old Karoonda Road turn-off just over the bridge, out of Murray Bridge. Inevitably, one would get behind a truck going up the old German Town Hill. It took me one and three quarter hours in travel time and so we would start the operation at about 1.00am, finish around 2.00am, have a cup of tea and head for home, arriving about 4.00am, three hours sleep and off to work at 8.00am. General surgery was highly competitive in those days and one could not knock work back – nor could one afford to have cases go wrong.
Workers Compensation cases were a godsend in the early days. I would spend one half of each day in charge of the Casualty Department at TQEH where my bread and butter came from finger injuries from the nearby factories. Skin grafts and cross finger flaps were my mainstay. It made sense to put these cases into a nearby private hospital rather than clog up TQEH theatres which were overloaded anyway. Under the WCA Act, the workers were entitled to private treatment.
I thought the Casualty Department ran fairly efficiently. It did annoy me that many of the migrant patients tended to treat it like a GP service, as they had been accustomed to in Europe. I did make strenuous efforts to discourage this but hospital management was disinclined to support me and so we were forced to live with it in the end.
Interestingly, the charge sister in Casualty was a Sister Sylvia Vaymos who had beaten Sadie, my wife, into second place in the State Midwifery exams! She ran the nursing side very efficiently.
All my private referrals were seen at 94 Ward Street together with the WCA cases but with four consultants sharing the one consulting room it was very squeezy. Colin Paull, Trevor Pickering and I had to engage two secretaries and so this, too, put additional pressure on available space.
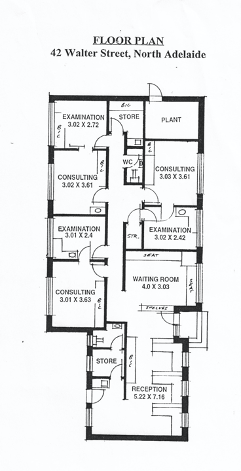
After a year or so, Colin, Trevor and I decided to move into our own rooms and we engaged a developer to find a block and build consulting rooms in North Adelaide. He door-knocked up and down Walter Street in North Adelaide and eventually had a response from an elderly lady leaning over her front fence. She made him promise to retain her old dwelling and I understand he did make that promise. However, she had no sooner completed the sale than the house was bulldozed and the new foundations for our rooms put down.
We were very pleased with Claude Parkin’s design, the builder he used and the materials, particularly the blackwood timber finishes. It comprised three consulting suites, office space for four secretaries, two toilets and a urine testing room and we were very happy when we shifted in around 1971.
Then we had to decide which of the three of us would have which of the three suites. We decided to each write on a piece of paper our preference and extraordinarily each of us chose a different consulting suite so everyone was happy.
We set up our rooms carefully and put the ownership in our wives’ names. Our wives then set up a managing company, Nasmec P/L, into which we paid rent and which paid all the expenses including secretarial wages and so forth. The profits from Nasmec were distributed to our wives who were also paid by us for secretarial work and after-hours phone minding for GP calls. The only defect that we had in our arrangement was that we each paid equal costs for the running of the rooms whereas we each had different demands on say, secretarial services, depending upon whoever had the busiest practice. Nevertheless, on the other hand, it was an incentive for each of us to get off our backsides and nurture our individual practices for which we retained full remuneration.
We were also careful to put into our personal agreement the process to be followed when one of us wished to retire and be paid out by the remaining partners. The rooms were to be valued by a nominee of the current President of the Real Estate Institute of SA with one valuation only to be made and this valuation to be abided by all parties. We were conscious of disputes which had arisen when both interested parties had obtained individual valuations.
There were huge advantages in having three of us working together. For example, Colin and I enjoyed a golf afternoon once a week, so each of us ‘looked after the shop’ for that afternoon so we could focus on our putting undisturbed.
Over the thirty or so years that Colin, Trevor and I were in our loose partnership, we never had one disagreement in our regular practice meetings. If an unpleasant task arose, such as having to fire an unsatisfactory secretary, Trevor and I would vote for Colin to do the job as he was the oldest and the most ‘fatherly’. On the few occasions this was found necessary, Colin did it well, with both he and the unfortunate secretary shedding a tear!
The other piece of good fortune which came my way on entering private practice was the appearance of an advertisement in the medical press for emergency surgeons for the Adelaide Children’s Hospital. There were three surgical units at the ACH and the three paediatric surgeons felt the emergency demands on them were too heavy, and they needed to share the load. I applied and, together with John Cox and Trevor Pickering, we became the ACH emergency on-call surgeons for rostered nights. I was allocated to Joe Savage’s Unit and found him a delightful person with whom to work. I had been used to working in hospitals in England where there was no distinction between children and adults. The cases we were called upon to deal with were refreshingly different to adults. We had the odd pyloric stenosis and, on one memorable night, I managed to score two intussusceptions.
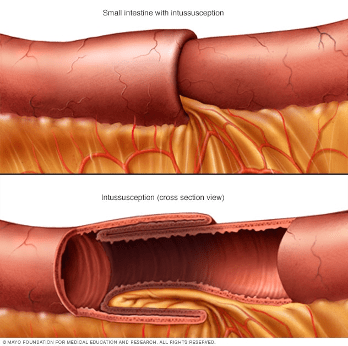
Small intestine showing intussusception
At that time, 1969-70, radiologists had become interested in this condition and were trying to reduce the intussusceptions by gently introducing barium rectally and gradually increasing the pressure. The radiologist had a go on the first case but did not succeed, or perhaps grew nervous as to how much pressure was permissible. In the end, we reduced it surgically, and when the second one arrived we did not invite the radiologists to have a go.
Joe was an interesting character. On another occasion I was called in to see a very sick child in renal failure, the cause of which I cannot recall. The understanding on the clinic was that if I had any problem, or the child was in danger of dying, then the senior would be called. Joe came in about midnight, by which time the child was resuscitated with appropriate drips and so forth and was stable. I could see no further point in us staying as there was nothing more to be done. I thought we should both return home but of course remain on call for any deterioration. Joe politely told me to go but he elected to remain at the child’s side for the rest of the night. A year or two later I was told Joe had decided to leave surgery and take up Nuclear Medicine as the pressure looking after sick kids was proving to be too much for him.
Meanwhile in 1968, back at TQEH, Noel Bonnin decided to retire, which meant there was an Honorary surgeon’s position available. John O’Brien was the next senior surgeon and so he took Noel’s place as head of unit on the fourth floor. It meant that John’s place on the fifth floor in Bob Magarey’s Unit was now available.
Competition for these posts was always very intense. Although unpaid, they gave access to a teaching hospital with its academic status, students, contact with top surgeons, latest advances in all specialties and public operating. One would be responsible for emergency surgical admissions about one night every week and have an individual operating list each week. There were two weekly full ward rounds with students and registrars attended by the three Honoraries and open discussion on the management of all the cases in the ward. All in all, very stimulating and exciting.
I do not know how many applied for the appointment but it would have been everyone at my stage trying to get a foot on the lowest rung. Trevor Pickering would have been the preferred candidate but he had already accepted a Senior Lecturer’s appointment to join Jim Harris in the newly developing vascular area, part of the University Department of Surgery.
Interviews were held, attended by all the heads of Unit but no announcement was to be made until it was approved and appeared in the Government Gazette. However, never able to keep a secret, Bob Magarey took me aside one day and told me I had the job. I would be joining Donald Beard and himself on the fifth floor. Perhaps a little disproportionate aesthetically, with Bob and Don both something over six feet six inches and me at five feet nine and a half inches, or so the Amateur League Football Budget proclaimed.
One person I did feel a little sorry for was Mark Sheppard. Quite justifiably, Mark felt that he should have been appointed to the Honorary staff when the hospital was set up. At that stage, he was in general practice on Woodville Road with John Waddy and Alan Lyle; the practice my family had used when I was a child as we lived across the road in Lesley Street. In fact, Mark had been our family GP of choice. The previous senior partner was Ross Morris whose son Richard was a playmate of mine. We played tennis on each other’s grass tennis courts in summer and kicked a footy there or in Jenkin’s paddock up the road in winter with the rest of the ‘Kelly Gang’ as my father nicknamed us.
Just as an aside, we also formed a local cricket team when we were all about fourteen, and used to play against another team from the south side of the railway line. We were on the north side. I remember we dug out a cricket pitch from the hard clay in Jenkin’s paddock which was a huge open space on the corner of Torrens Road and Hughes Street. For the return match, we went over to the southern side of the railway line where the ‘southsiders’ used an area in Connors’ extensive grounds, the site of the future QEH. Interestingly, the opening fast bowler for the south side was John Drennan, who went on to play for Woodville, South Australia, and toured South Africa as Australia’s fast bowler in 1957-58. John also toured New Zealand. He had honed his skills against us poor kids in Jenkin’s paddock as a very tall fourteen-year old and even at that stage he was very fast with the balls bouncing anywhere – no helmets of course.
I happened to look after John’s father as a public patient at TQEH years later and bumped into him in the ward, so we shared those early memories. John was Town Clerk of Port Adelaide Council at the time, if I remember correctly.
John Drennan
The captain of the South Woodville team, Brian Crompton, was a friend of mine and perhaps the two of us may have instigated the original cricket challenge. We used to catch the 8.10 am train from the Woodville Railway Station together and often the notorious 4.10 pm train from the Adelaide Railway Station. Notorious, because it was bound for Semaphore and was filled with private school kids from all the colleges, male and female, on their way home to the western suburbs.
There were no elite colleges in the western suburbs in those days – ‘western suburbs people’ were not supposed to be able to afford to give their kids a college education. The 4.10 train was always ‘dog boxes’ – that is, each carriage was comprised of about eight separated compartments, each with a door opening directly onto the platform. To board the train at Adelaide Railway Station, one had to present one’s ticket at the gate and then walk the length of the train in order to find a ‘friendly’ compartment – with all the kids hanging out the windows watching and cheering. If you were bold, you chose a compartment full of girls but this was rare.
In later years, when I was an impecunious medical student, I bumped into Brian on the morning train one day and we engaged in conversation. I told him I was looking for a Christmas holiday job and he offered me one. He told me he was auctioning kids Christmas toys in an auction room in the city every Saturday morning. I did not question how this young lad of about twenty came to have such a job as I was desperate for work. He told me he would pay me £10 a morning and my job was to mingle with the buyers and, as he auctioned each job lot of toys, when he looked at me I was to put up my hand and make a bid. A stooge, if you like, but easy money and I accepted.
On the following Saturday morning, I presented myself at the appointed auction rooms and followed Brian and his group of buyers around bidding for separate lots of toys as he looked at me. However, I think he was looking at me far too often as the rest of the bidders started to look at me and grumble as they realised I was a stooge and so I was forced to lay off for a bit. He and I clearly had to improve our system in order to make it look genuine. Anyway, he did pay me £10 for my morning’s work – good money at the time. On reflection, I thought better about returning for another Saturday and pursued other, more honest, avenues.

Captain Mark Yeatman Sheppard WWII Image: Virtual War Memorial Australia
Returning to Mark Sheppard. He passed his FRACS (surgical qualification) whilst working in his general practice and learned his surgery under the old apprentice system by assisting experienced surgeons. He did all the surgery in his practice and operated for a few other general practices in the area and was very competent. When TQEH opened, the seventh and eighth floors were designated as private and, after a deputation from the surrounding general practices, these practices were given admitting privileges and operating rights in the hospital. Mark was operating in TQEH from its inception. Unfortunately for him, the day of the apprentice surgeon had passed and he was never appointed. In later years, I did have the privilege of looking after his varicose veins practice in Ward Street whilst he did a three months stint in a surgical team in Vietnam.
Mark contributed greatly to the medical profession with a term as AMA State President, was always a perfect gentleman – and recently reached 100 years of age!
With my appointment as an Honorary Surgeon, my future career was somewhat laid out and predictable.
Once a year the surgeons of Adelaide had an annual dinner at the prestigious Adelaide Club organised by the College of Surgeons. As an impending appointee to TQEH, I received an invitation in 1969.

The Adelaide Club, North Terrace
The Adelaide Club began in 1863 and was exclusively for men. In fact, ladies had to enter by the side door if they were invited to dinner. The concept was based on the old private members’ clubs of London, originally coffee houses, which became popular after the beverage was introduced into England from Turkey by David Saunders in 1652. These clubs in the nineteenth century were places where gentlemen could find ‘refuge’ from their womenfolk in a private building which resembled a stately mansion. In the 1960s, the Adelaide Club had been entertaining an elite membership for 100 years but, by 1969, its exclusivity was waning.
The Adelaide Surgical hierarchy seemed not to have progressed from the nineteenth century and many still believed the Adelaide Club was where the ‘important’ decisions were made.
On the occasion of my invitation, I attended the gathering and, as usual, it started with pre-dinner drinks. Wow! Champagne Cocktails were being handed out. As a poor, impecunious registrar, I could never afford such luxuries. So I had one and then a second and felt decidedly better. Perhaps I had a third, I don’t remember. On the other side of the room were the ‘doyens’ of Adelaide surgery, RAH-based Alan Lendon, discussing surgical politics with Sir Leonard Lindon. Alan Lendon did not know me as I had only worked at TQEH and, as I had just been appointed to a senior position, he wanted to make my acquaintance. He sent one of his minions to fetch me and I duly joined him and Sir Leonard. Well, trying to differentiate between Alan Lendon and Sir Leonard Lindon would be a tongue twister at the best of times but after two or three champagne cocktails the inevitable happened and, to my horror, I deferred to Alan Lendon as ‘Sir Alan’. To my complete surprise, he beamed – ‘Sir Alan’ was music to his ears. He chortled and put his arm around my shoulders and declared, “Not yet, my boy, not yet!” In fact, the knighthood never did materialise.
I was duly seated next to my old mate, Tony Slavotinek, and Russell Barbour sat next to him on his other side. As soon as Tony sat down, he reached for his fags and then found he had no matches. He turned to me, “Got a light Ross?” “I don’t smoke Tony,” I replied, whereupon he turned to his other side, “Excuse me Sir, have you got a match?”

Russell Barbour was one of Adelaide’s most notable surgeons, an orthopod by choice, but he would often have other operations on his list such as the odd hysterectomy. He taught us anatomy and was undoubtedly one of Adelaide’s most talented surgeons in his generation For a fractured Colles he would say, “Always put your dorsal slab on the ventral surface!”
Antonin (Tony) Hynek Slavotinek. Image: SA Medical Heritage Society
On this occasion he replied to Tony, “No, I’m a Queen’s man myself” meaning that one does not smoke before the loyal toast to the Queen has been proposed. Tony, a Czech originally from Prague, turned to me and asked, “He says to me he’s a Queen’s man. What does he mean?”
It was a night of firsts and I began to feel much better about my own faux pas.
It was part and parcel for GPs to have private lists at TQEH on a regular basis in those early days – usually simple things like tonsils and adenoids and such like. If they wished, they could consult any of the Honoraries, so it was to everyone’s mutual benefit. Inevitably though, there were a few cowboys who ran into trouble, biting off more than they could chew, resulting in serious surgical complications. As a result, the practice lapsed and, eventually, the two private floors were only used by hospital staff.
I looked forward to the experience of working with Bob. I credited him with my appointment, believing he would have had the final say in who would be allocated to his unit. Although he never confided in me, I feel sure he would also have been relieved to see the departure of John O’Brien to be head of unit on the fourth floor and who had not enjoyed being second-in-charge.
On reflection, over 50 years after the event, I appreciate how instrumental Bob Magarey was in helping me achieve significant milestones in my career. Firstly, my student contact with him in organising the medical dinner in sixth year, secondly being appointed as a Senior Registrar at TQEH, thirdly passing the Australasian Fellowship and, finally, my appointment as an Honorary Surgeon at TQEH. Without his help in pushing my barrow, I may not have achieved any of these milestones.
I enjoyed my time working with Bob on his unit. He treated me with kindness and respect at all times. He was himself very ambitious and had hoped to be elected President of the Royal Australasian College of Surgeons, an appointment which he would have held with great distinction. However, I believe that due to petty jealousies within the college, he was not chosen and so thereafter spent his energies pursuing appointments with the Australian Medical Association. He was very successful in this area being elected State President and, finally, Australian President.
Bob Magarey chairing a meeting of the AMA

The third Honorary Surgeon on the Magarey Unit was Donald Beard. Sometime around 1973, Don was offered the appointment of Surgeon in Charge of Surgical Services at the recently built Modbury Hospital and so he left. My good friend of many years, Trevor Pickering, decided at that stage to return to General Surgery from Vascular surgery and so he was appointed to Don’s place. I was very pleased at this turn of events as, I believe, was Bob.

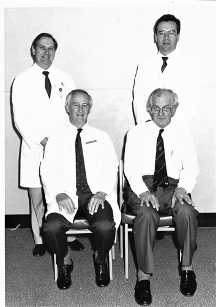
The Magarey Unit: The author, Trevor Pickering and Bob
Bob rarely talked of his WWII exploits and his experiences in the Syrian Campaign or on the Kokoda Trail, nor did he tell us that he had been mentioned in despatches in the Syrian Campaign. Various books have described his war exploits, including Retreat from Kokoda, No Memory for Pain and Those ragged Bloody Heroes.
It is to the everlasting credit of Magarey, his staff, the RMOs, the native carriers and the troops themselves, that not one wounded digger known to them, was left at the scene of the battle during this whole campaign.
Peter Brune, Those ragged Bloody Heroes: From the Kokoda Trail to Gono Beach, p. 129
I wrote the following footnote regarding Bob Magarey for Bill Proudman’s history of TQEH[1]:
Bob was State President of the AMA in 1970 and was the chief negotiator with the State Government to change the Honorary system to one of paid sessions. He was always a tough and skilled negotiator. I remember him coming into the morning tea room after a ward round on one occasion at this time and, taking up a position in front of the blackboard with chalk in hand, he discussed with Don Beard and me what he felt were reasonable estimates of our workload. Yes, I felt at the time that we padded it out a bit but then, on reflection, appreciated that, in true union style, one should always start with the ideal and negotiate backwards from that position. A few days later, Bob forwarded to Don and me the final document for our perusal. To his credit, he negotiated successfully for the surgeons to be paid for five sessions (17.5 hours) per week and the physicians for four sessions (15 hours). He did not have to, nor would he ever have, taken any backward steps with the bureaucracy!
Final stage of the document presented to TQEH Medical Superintendent arguing for changes to Visiting Staff conditions. Ibid [2]
Bob contributed hugely to TQEH and filled all the important posts in due course. I was disappointed to hear disparaging remarks made behind his back by some of his colleagues from time to time, despite them benefitting greatly from his efforts. When he received the news of his knighthood, there was not the uniform acclamation from his fellow surgeons at the hospital as there should have been. Trevor and I, together with our wives, took it upon ourselves to give him a special evening and made a small presentation, and he was very appreciative.

Sometime in the mid-seventies when Bob was President of the SA branch of the AMA, the secretary, Ian Furler, took ill and had to resign. I remember Bob coming into my consulting room in outpatients and relaying this distressing news. It ended with him offering me the job on the spot. I don’t think I was even a member of the AMA at the time and I certainly had no wish to take on further commitments. On the spur of the moment I said, “I’m not very good at those sort of jobs Bob but I know who would do the job very well – and that’s Trevor Pickering.” At that moment Trevor was consulting in the outpatient suite next door.
“Trevor, yes of course,”said Bob. “I didn’t think of him. I’ll ask him.”
With that, he went next door to Trevor, who accepted the offer, and so began Trevor’s very successful career in medical politics, culminating in him becoming Federal President in 1985 and being awarded the AMA Gold Medal in 1992.
Bob Magarey was generous to a fault and entertained the whole unit on a regular basis, both at his home at Medindie and down on his farm at Mt Compass where he would hitch up his tractor to a hay wagon and take our children for rides. He gave of himself to his colleagues and certainly Trevor Pickering and I have very fond memories of the man himself.

Captain Magarey with wife Mary taken during WWII. Courtesy SA Medical Heritage Society
How sad it was for Bob and and his family when his beloved Mary died in the late 80s. Bob had developed dementia before she died and I visited him at the College Park Nursing Home shortly before his death in 1990 at the age of 76. He was still at that stage a strong, fine looking man, upright, and with a full head of dark hair, well dressed in a tweed jacket and proudly wearing his college tie. He looked so out of place amid the crumbling humanity around him. We had a good chat about old times and then said our farewells for what would be the last time.
Returning to my private practice, a big event occurred serendipitously in the early seventies. One of my very best friends, Frank Altmann, had settled into general practice at Murray Bridge in the mid-sixties, joining Fred Heddle and a surgeon, Vic Springett. Vic had become a Member of the Legislative Council but the practice found the arrangement was not satisfactory as the demands of parliament meant he was not always available when needed for surgical emergencies.
Around the time Vic Springett left, David Haines joined the Murray Bridge practice. David had done some postgraduate training in anaesthesia and introduced intubation and other more advanced techniques. Frank approached me to take on the Murray Bridge surgery as a weekly visiting surgeon.
My response was that I would find it difficult to provide an effective service on my own as I was still half time employed in TQEH Casualty Department. I suggested that Colin Paull, Trevor Pickering and myself could provide a good service by sharing the load and each spend a day in the bridge each week, operating in the morning and consulting in the Murray Bridge Clinic in the afternoon. We would take it in turns being on call for emergencies week and week about.
I approached Trevor and Colin to see if they would be agreeable to such an arrangement. I felt the standards of the three of us were on a par and there would be no disagreements on the management of surgical problems. It would mean that the operating surgeon would not necessarily be the one who saw the patient initially but I saw no problem with this.
The Murray Bridge doctors were enthusiastic about accepting this arrangement, especially as it meant they would have a connection to a teaching hospital and we would arrange for transfer of the more difficult cases unable to be dealt with at the Bridge.
And so it came to pass that, for the next 30 years, we provided an effective surgical service to the Murray Bridge Hospital. As the practice in Murray Bridge grew, they expanded the visiting specialist group to include ENT, Eyes, Orthopaedics, Cardiology, Gynaecology and others. Starting with three GPs, their practice grew to some fourteen or fifteen by the time we passed our service on to the next generation. The Murray Bridge Clinic now comprises 25 doctors and is a centre of excellence. The incumbents in the practice were well able to deal with all the minor surgery, appendices and so forth.
We did have the occasional interesting situation when a GP would diagnose an appendicitis only to find it was a cancer of the right colon. We would get an urgent call to let us know. What to do? Well, the anaesthetist would keep the patient asleep while one of us would jump in his car and hotfoot it up to the Bridge (one hour plus), scrub and gown up, confirm the findings, resect the bowel, have a cup of tea and go back home. It made life interesting.
I can only remember one anxious moment on an operating list when the gall bladder I was scheduled to remove turned out to be hot (acute). This in itself did not make the situation necessarily more difficult but, on tying off the cystic artery, the tie went through the artery like butter and the wound filled with blood. Well, that did make it difficult as we were not in the habit of grouping and matching blood for patients for simple cholecystectomies, although in earlier years in surgery this had been routine.
One of the dictums of surgery is that a bleeding vessel, even a large one, will contract with time and patience and slow to a trickle eventually and all is salvagable. Nevertheless I remember saying to Bob Cowham, my anaesthetist (and a very good one), “Oh mother, why did I ever leave home!”
The technique involves packing the wound with large sponges, perhaps three or four and then leaning on them. As these sponges become saturated, they are removed and replaced with fresh ones. Fortunately, we had the facilities for rapid cross-matching of blood at the Bridge and Bob sent blood off pronto. To make matters worse, the patient was a close family friend of my assistant for the day, Frank Altmann.
After 30 to 40 minutes, the speed with which the wound was refilling noticeably slowed and so the packs were gently removed and, using gentle suction, the offending vessel could be identified in the depths of the wound and, ever so gently, a ligature was tied around the it and the wound closed.
A cup of tea was very welcome before we continued with the rest of the operating list.

Bridge Clinic, Standen St., Murray Bridge, with the old original House where we started consulting in the late 1960s at the right side of the image.
Those were the days when general surgeons did everything and so our lists at the Bridge included a sprinkling of orthopaedics, including menisectomies, for which we had to purchase special instruments. The biggest procedures we did up there were cholecystectomies so we had to buy a choledochoscope. Eventually, in the mid-nineties, we moved to doing them laparoscopically. We opted not to do bowel procedures at the Bridge as we thought those would be better done in town where we could keep a closer eye on them postoperatively.
Bill Proudman’s retirement in February, 1993, was a big loss to TQEH. Bill became the first Honorary appointed who had trained under the registrar system rather than the old apprentice system. Bill’s time at TQEH represented the halcyon days of the hospital. Having been there from the hospital’s inception, Bill was able to create a tradition and environment of excellence and trust which pervaded the institution and infected all those who worked there.
In my Foreword to Bill’s book[3], I wrote: The hospital in those days was without doubt the centre of our professional lives and our private practices were secondary. We had no qualms about attending Saturday morning outpatients (unpaid as Honoraries) followed by an Alan Kerr Grant gastroenterology seminar at 11.00am. We enjoyed our Thursday lunchtime Grand Rounds attended by the whole medical staff, including nurses if they wished to come. We had monthly Deaths Review and the social functions were always well attended, and included our wives.
Bill initiated a number of novel ideas when he took over as Head of Unit with Bob Magarey’s retirement in 1979, one of which was a ‘Lumps and Bumps’ session on a Saturday morning, held once each term for the students.
TQEH Surgical Outpationts
Over the years we collected a number of one-off patients on a register with interesting and unusual clinical signs who would be happy to give up a few hours of their day. They would be examined by all the students in turn and then discussed in the lecture theatre afterwards. It was very popular and attracted large numbers of students from all the teaching hospitals in Adelaide, and also fellowship candidates. The patients themselves patiently endured the ordeal – all for a cup of tea.
When Bill became head of unit and I was one of his subordinates, he introduced a weekly radiological program with a review of all the week’s xrays – and also a weekly pathology session with review of our week’s specimens and slides. Everyone attended, including our students. They were good learning sessions for us all.
The Proudman Unit – Bill with author (seated) Trevor Pickering and Vlad Humeniuk standing
[1] WD Proudman, In the beginning: The formative years of The Queen Elizabeth Hospital, p.79
[2] ibid, p.82
[3] ibid, p.iii
READ Chapter 15
