
The Professorial unit
Every twelve months, the three senior registrars rotated to another unit. In 1967, I was allocated to the Professorial Unit, the University Department of Surgery. A few notes follow on the history of the Department of Surgery at The Queen Elizabeth Hospital.
Dick Jepson was the first Professor of Surgery in Adelaide and the Chair is now named after him. Adelaide was extraordinarily lucky to obtain the services of such a high calibre surgeon as Dick Jepson. He already had a Chair in Surgery in England at Sheffield University – so why did he decide to leave and come to a comparative backwater like Adelaide?
The answer that I have been given is that, with four daughters, he felt Australia would be a better place to bring them up. He arrived in Adelaide in 1958, some nine years before I joined the unit.
Dick was a pioneer in vascular surgery and introduced that specialty to Adelaide. He was a master technician with a first-class brain and he lifted the standard of surgery, not only in Adelaide, but with an influence felt across the whole of Australia.

Professor Richard Pomfret Jepson
Dick Jepson graduated in Medicine at Manchester University, where he was awarded blues for cricket and golf.
Two years after the outbreak of World War II, he became a member of the No. 5 Neurosurgical Unit headed by Sir Hugh Cairns who had graduated in Medicine from Adelaide University, later travelling to Oxford on a Rhodes scholarship. One of the fathers of penicillin, Howard Florey, had followed a similar path from Adelaide to Oxford with a Rhodes Scholarship, and both would have a significant impact on Jepson’s experience of wartime medicine.
From The Royal Australasian College of Surgeons History Project [1]:
The initial training of Jepson’s Neurosurgical Unit was at Oxford. In December 1942, the unit sailed from Liverpool for Algiers and a small hospital at Sousse, on the Mediterranean coast in Tunisia. The casualty rate was considerable and the incidence of infection high. Head injuries and spinal injuries were dealt with in tents and sterilization was by boiling, using primus stoves.
It was at Sousse where the team was visited by Cairns, Florey and his technician. They
brought their first consignment of Penicillin. It was only a small quantity made in Oxford. Cairns and Florey supervised the intravenous doses. It was probably the first time Penicillin was used to treat combat casualties. The results were miraculous.
As the war progressed Jepson’s unit became part of the 8th Army and followed the campaigns through Italy finally ending in Florence. By the end of the war Dick had learned sufficient Italian to later settle a dispute between the Italian workers and the management of the Queen Elizabeth Hospital.
Returning to Manchester after the war Dick married a young medical student, Mary Oliver, daughter of the Professor of Medicine. He was appointed to the Chair of Surgery at Sheffield University in 1954, and in 1958 at the young age of 39 he accepted the appointment as Foundation Professor of Surgery at the University of Adelaide and in that same year travelled to Adelaide with his four daughters.
The newly built Queen Elizabeth Hospital was his first base. The reason for choosing that hospital was the presence of modern equipment, young staff and a well-equipped animal house. Here he assembled an enthusiastic team of surgeons and researchers. The facilities of TQEH Animal House were ideal for teaching vascular surgery and performing renal transplantation on dogs. This research resulted in the first Australian renal transplant from a living donor…and was performed at TQEH in 1965 by Peter Knight with Bill Proudman on the donor side.
Transplants were performed on a regular basis thereafter. Donors were much in demand and physicians of the renal unit were said to be doing the odd ward round in ITU to assess those patients close to death whom they anticipated could become likely donors. Of course, that rumour might have come from the surgeons themselves, who did like to stir the pot.
These transplants were not without their hazards as many of the subjects were hepatitis B carriers, a result of repeated dialyses. In fact, two senior surgeons involved in the transplant teams contracted hepatitis B infections – Peter Harbison and Trevor Pickering – necessitating long periods off work to convalesce. I understand that these infections were eventually accepted as being work-related and they were compensated. Sadly, one of our popular and talented junior registrars at that time, Richard Welch, also contracted hepatitis B and, after a protracted stay in TQEH, it claimed his life. I don’t know whether he had been in contact with the renal unit. Richard’s father, Frank, was an Obstetrics and Gynaecology consultant at TQEH and he and I later shared operating duties at Karoonda in country South Australia. Richard had three siblings, all doctors. His passing was a big blow to all of us at TQEH.
Dick Jepson was recognised Australia-wide for his surgical expertise and academic skill. He changed the face of surgery in Adelaide.
In 1965, Professor Jepson changed his base and moved his Department of Surgery from TQEH to the Royal Adelaide Hospital, leaving his Reader, Lou Opit, to run TQEH branch. I started at TQEH the following year and so saw very little of the Professor. On one occasion, Colin Paull encountered Dick Jepson in the corridor and suggested he may be interested in an aneurysm I was excising from the lateral plantar artery. The great man entered the theatre, looked over my shoulder, grunted and departed.

Louis Jonah Opit, image courtesy of SA Medical Heritage Society
One of Dick’s innovations was to set up a Surgical Forum to be held every Tuesday lunchtime in a seminar room to discuss a wide variety of surgical topics. Everyone in the hospital was welcome. I remember on one occasion in 1967 there was a debate on thyroid surgery. Professor Jepson, who was an international authority on thyroid disease, found himself in a vigorous discussion with his Reader and junior, Lou Opit. Lou loved an argument and usually took an opposing view just for the hell of it. On this occasion, Dick took exception to Lou’s strong language and suddenly announced, “Well, clearly, this hospital has no need of my input!’” – whereupon he left the meeting, and the hospital, never to return. Lou was left to run the University Department at TQEH on his own. I would not imagine that Lou ever apologised for the hurt he caused, it was not his style.
Each month, one of the Surgical Forums was dedicated to a ‘Deaths’ Review’ – discussing in detail one or two surgical deaths occurring during the previous month which may or may not have been preventable or better managed. These were chosen by the pathologists who of course, were responsible for the autopsies carried out each month. Taken as a teaching exercise, these sessions were highly instructive and tended to be ‘sell-outs’ on their day. However, as time went by, they became ‘Coliseum’ events, with the Christians being thrown to the lions and so, sadly, for the sake of harmony between the surgeons and physicians, these events were discontinued, with each surgical floor conducting their own monthly deaths reviews internally.
Dick was a strong believer in opportunities for younger talent and so retired early in 1968 and set up a private vascular practice with Jim Harris. He died from cancer of the stomach at the young age of 62 in 1980.
A final anecdote comes from his partner in surgical practice Jim Harris;
I knew that he was a good golfer and I believe that there was a professional golfer who lived nearby (in Manchester) who taught Dick during his holidays. I was surprised that a golfer of his calibre could give the game away as he did when he came to Australia. Many of us, however, remember an annual AMA tournament. He arrived at the first tee at the Royal Adelaide Golf Club with a set of old wooden golf clubs in his shoulder bag. Having secured a handsome handicap, he proceeded to tear the field apart and left his partner, John Maddern, also a good golfer, in a state of shock.[2]
Dick Jepson’s replacement as Professor was John Ludbrook from Sydney. He based himself at the RAH. As part of his appointment package, he brought with him as his deputy Ron Elmslie, who was appointed Reader and based at TQEH – without any input from TQEH and its staff. This in itself was not a good start for Ron Elmslie.
Lou Opit had already resigned from TQEH in 1968 allowing Ron Elmslie to take over the Department of Surgery as Reader. When a Chair of Surgery was eventually established at TQEH, Ron Elmslie applied but was denied appointment on two occasions. He was finally appointed to the Chair in 1975, based entirely at TQEH. His tenure as professor was not successful. He was not the leader of a vibrant department where research flourished and seemingly did not particularly enjoy operating, as his appearances in theatre were spasmodic. He did not enjoy rapport with the visiting staff and kept his department very much separate from the rest of us. All in all, it was not a good period for surgery at TQEH and it was with some relief possibly for him and certainly for us that he eventually retired around 1992. Ron retired to the Southern Vales, south of Adelaide, and died in 2003 at the age of 71.
Ron’s successor in the RP Jepson Chair of Surgery at TQEH was Guy Maddern, who took up his appointment in 1993 at the young age of 36. His impact was immediate and the rise in morale among the surgical fraternity at the hospital was palpable. He was young, dynamic and created a vibrant research atmosphere attracting significant research funds to his department which was refurbished on the sixth floor of the hospital. He gathered around himself in the Department of Surgery Tony Slavotinek, Frank Bridgewater and Peter Byrne, all of them highly respected by the other visiting surgeons. Originally, the Professorial Department of Surgery included Bill Roediger but ,with the subspecialisation of three units, Bill chose (or was sent by the Professor to) the Colorectal Unit.
Guy had first come to us as a Junior Registrar in 1987 when Bill Proudman was head of that unit. At that stage, he had just completed his PhD as I remember and was short on operating experience. Guy was the son of a prominent urologist, which usually was a disadvantage in Adelaide, but John Maddern was universally liked and respected and surgical jealousies were fading into the past. Certainly, at TQEH where we had the younger brigade, it was not a problem.
Guy, as I remember from that year, 1987, made himself a regular pest. It was the duty of the junior registrar to organise the admissions for our operating lists and write them up on the blackboard while we had cup of tea after the regular ward rounds. Guy’s call-ins presented us with operating lists which would take six hours of very slick operating rather than the four hours we were allocated. Being a teaching hospital, we used some cases for the senior surgeon to assist his juniors and so Bill, who was no slouch with the knife, had to bring him back to the real world.
So much for the historical background of the Department of Surgery at TQEH over the years. When I arrived in 1966, Professor Jepson was spending most of his time at the RAH, leaving the day to day running of TQEH unit on the second and third floor to Lou. In running his ward, I answered to Lou.
The South Australian Medical Heritage Society notes that Lou Opit was born in Curramulka in South Australia. His father, Leon Opit(z), was a general practitioner in Curramulka and later Torrensville and a respected member of the Adelaide Jewish community.[3]
My first contact with Lou had been when he was Sid Krantz’s senior surgical registrar at the Royal Adelaide Hospital. I was a sixth year medical student and it was clear to us that Lou and Sid had a good rapport – perhaps because of their cultural heritage. They had similar temperaments; both were outspoken, loud and confrontational. Sid had made his mark as a surgeon on the Burma Siam Railway during the war and often deferred to Lou when faced with highly academic questions. Needless to say, they were both unusually highly intelligent for surgeons.
My time with Lou was memorable. He was only six years older than me and was full of fun. A lateral thinker and a lively and humorous contributor at surgical meetings, he took delight in belittling physicians. He would always take the opposite side of an argument, any argument. Technically he was a good, competent surgeon, with good hands.
I could detect that even at the young age of 40, he was starting to find surgery boring, and meetings and ward rounds frustrating and tedious. When I joined the unit, he had already attached himself to the Department of Mathematics at Adelaide University and was immersing himself in biochemistry with a biochemical scientist attached to the Department of Medicine, John Charnock. Together, they made a significant scientific discovery which was published in Nature in 1965: ‘A Molecular Model for a Sodium Pump’. Another of his best scientific papers on ion transport, also published in Nature, was reported to have been written over a bottle of red wine.
Lou was a restless, loose cannon. His notorious confrontation with his boss, Dick Jepson, which led to the Professor’s walkout was typical of Lou’s provocative ‘know all’ approach. Yet, he bore no malice after such arguments and was admired and well-liked by all the other surgeons in the hospital.
Lou had been personally responsible, together with Dick Jepson, for persuading New Zealand surgeon Peter Knight to cut short his return from a job at Massachusetts General Hospital to join him instead at the University Department at TQEH.
Peter had trained as a transplant surgeon in the US and, because the Queen Elizabeth Hospital had a functioning animal house set up for experimental surgery, Peter was persuaded. In 1965, the year before my arrival at TQEH, he performed the first successful kidney transplant from a live donor in Australia.
Peter was a delightful person, extremely talented, and I spent many happy hours assisting him in the animal house as he perfected his technique. Later, we moved on to developing techniques for liver transplantation. The sacrificed pigs were divided up between us as roast pork for our evening meals.
The liver transplants never came to fruition as Peter eventually found he was unable to work with his corresponding physician in charge of the renal unit at The QEH, one James Lawrence. I had played football with Jim in the Uni ‘A’s some years before and knew his shortcomings very well. He would try to direct the proceedings of the team from the half-back flank but nobody took any notice. Jim always called me ‘Ripper’, a nickname from our footy days. His manner irritated Lou Opit, who commented that in meetings and seminars…” Jim would stand up and say, ‘yes, I completely agree with you’ and follow up by trying to totally dismantle your argument!”

Jim Lawrence – Chair of Medicine, Concord Hospital, Sydney
Jim sought a Chair in Medicine which wasn’t easy as he had narrowed his interests into Nephrology. Eventually, he took the Chair of Medicine at Concord Hospital in Sydney. Coincidently, my son David had a stint as his resident at that hospital in later years.
Regrettably, Peter later resigned and took up an appointment at McMaster University, Hamilton, Ontario, where he remained for the rest of his career. He was a huge loss to TQEH.
During my year on the unit, Peter thought he had better pass the Australasian fellowship so, in due course, he went across to Melbourne to present himself in front of the examiners. Unbelievably, they failed him, after asking some obscure pathological questions that he had long since forgotten. Here was Peter, a colossus striding across the surgical spectrum, belittled by his peers. His achievement in performing the first renal transplant in Australia should have in itself been worthy of an Honorary Degree. He came back to the unit very bitter and disillusioned and I believe that this experience also contributed to his unfortunate departure.
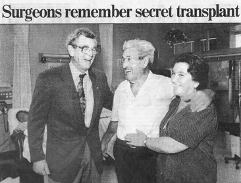

Above. Professor Peter Knight (left) with the first successful kidney transplant donor in Australia, Dominic Centafate, and his daughter Stella Tirimacco 30 years after the event (The Advertiser 24 Mar 1995). Below Professor Peter Knight shortl before his death in his mid 90s in 2018. Courtesy McMaster University magazine Ontario, Canada
I was responsible for the ward under Lou and Peter who were very close friends professionally and socially. We had great times and they treated me as an equal. On one occasion, Lou took it into his head to use a Boyles anaesthetic machine as a horse. The machines were on four wheels and Lou, dressed in his theatre garb, pushed it down the theatre corridor at some speed then mounted it and proceeded to belt it with a whip! Great fun for all, including the nurses.
I remember Lou for his happy demeanour, his short stature, his tight curly hair with dandruff and his perpetual blepharitis – red eyelids, with scales. In 1968, the year after I worked for him, he resigned from TQEH and returned to Warwick University where he had been a surgical registrar in 1953. There, he graduated BSc (Hons) in Applied Mathematics in 1969.
Lou had a dynamic and original mind. Would he have made a good professor of surgery? He was unpredictable and prone to making precipitous decisions. Life was never dull with Lou around. Was anti-Semitism still alive and well? Lou had already been passed over at the RAH in favour of ‘Frosty’ Hoare when he was a Senior Registrar at the RAH.
He never returned to surgery which he found formulaic and, frankly, boring. He was far too intelligent and creative to spend his life operating. He became a Research Fellow at Kings College Hospital in London in medical computing, then joined the Health Service Research Unit at the University of Birmingham before moving on to become professor of Social and Preventive Medicine at Monash University. He eventually returned to the UK after accepting a post as Professor of Community Medicine at the University of Kent. He was also a consultant to the WHO.
Lou had a total of eleven career moves. He thrived upon the challenge of uncertainty and felt the need to periodically reinvent himself. He was a restless soul. He was also something of a paradox. He was a Professor of Preventive Medicine but also a chain smoker and this eventually caught up with him when he developed pancreatic cancer necessitating a bile duct stent.
It was said of him by a colleague in Kent, “Lou’s unique brand of self-expression enchanted, instructed and provoked whoever happened to be within earshot.”[4]
Lou was devoted to his large family. He married Gwen Gartrell in 1952 but they divorced. When he died, he left behind a partner, Jan Pahl, four children and eight grandchildren in Australia and the United Kingdom. He died from his pancreatic cancer in Canterbury in 1998. During his life Lou did not give his friends any indication of his religious convictions but in his will left instructions for his body to be flown from England to Melbourne to be buried in the Springvale Chevra Kadisha Jewish Cemetery.
His partner, Professor Jan Pahl wrote:
During those years his love of his family and his Jewish loyalties were clear to all his friends. He would frequently quote from the Talmud: one of his favourites was, “If I am not for myself, who will be for me? And being for myself alone, what am I? And if not now, when?”. He attended the Jewish synagogue in Chatham, where, after he died his body was prepared for burial following the Jewish funeral rituals. His three children then living in England and I then flew with his body to Melbourne for burial in the Springvale Chevra Kadisha Cemetery. The names of his children and grandchildren, and my own name, are on the headstone of his grave.[5]

The final surgeon on this happy unit that I worked for was Jim Harris, at that stage Senior Lecturer in the Professorial Unit. He had been button-holed by Dick Jepson to enter the emerging specialty of Vascular Surgery and had been sent by Dick to spend a year with Michael DeBakey in San Francisco as his registrar. DeBakey was a legendary surgeon who transformed the practice of cardiovascular surgery.
Jim, as with all the surgeons on this unit, had extraordinary skills, such that when Dick Jepson retired from hospital practice into a private vascular practice, he invited Jim to join him as an equal partner. I had played with Jim’s older brother Digby, who was captain of the University A1 Football team (the ‘Blacks’) in 1953.
Jim died in 2018 – the very week his son Richard, an anaesthetist and cave diver, was to receive world-wide acclamation for his rescue of fifteen Thai boys trapped in a cave below ground. Richard was selected as Australian of the year for 2019.
Jim and Richard Harris
Everybody loved Jim. He had an infectious smile and laugh and was always ready with a joke. I never saw him in an ill humour. I had good reason to be grateful to him as he bailed me out of a tricky situation on one occasion shortly after I had entered private practice in 1968.
One of my referring GPs at Karoonda in the Mallee area, Ian Murdoch, sent his father to me. A very nice, retired company accountant, I had previously dealt with his inguinal hernia, one of the biggest I had ever seen, the size of a small football. On this occasion, I was looking after his prostate cancer, which had spread to the lymph nodes in the para-aortic area. Try as I may, I cannot remember how or why I found myself inside his abdomen on a Saturday night around midnight with uncontrollable bleeding coming from the venous plexus behind the IVC, infiltrated with secondary spread from his Ca prostate. I packed the area and rang my good friend Jim. He had just arrived home from a good party somewhere and was well lubricated. Without the slightest hesitation he jumped back in his car and set off down the Port Road. In quick time, with his vascular instruments, he mobilised the appropriate vessels and tied off the bleeders and left me to sew up. I was eternally grateful as, in those early days, I was very dependent on the steady flow of work I was getting from Karoonda.
During my registrar stint at TQEH in 1967, I had two interruptions to my hospital routine.
The first occurred when Bob Magarey as President of the SA Branch of the College, decided that it would be a good idea if the senior registrars had a stint in a country surgical practice and the country surgeons came into TQEH as a swap for, perhaps, one month. This would allow the country surgeons to get an update in their surgery and give the registrars a taste of country surgery. A good idea.
Bob nominated me to be the guinea pig so, in due course, John Smith from Naracoorte came in to take my place and I uprooted my family into our trusty Austin Lancer and moved into rented accommodation in Naracoorte.
We enjoyed our month and I found the work interesting and the GP anaesthetists to be of a good standard.
My most vivid memory of that month was having to operate on three cases of hydatid disease, rife in the southeast of SA at that time. I only remember the details of one case which sticks in my mind. It involved a young male patient on whom I performed a laparotomy, the indications for which I can’t remember. However, to my horror, his peritoneal cavity was riddled with hydatid cysts which I attempted to remove, injecting them with formalin before doing so. At the end of this tedious procedure I was closing the abdomen when the scrub sister announced that she was a swab short. I retorted that her count must be wrong as I never introduced loose swabs into the peritoneal cavity unless they were on swab sticks. However after further searching around the floor and under drapes, she persisted with her claim. Reluctantly I reopened the abdomen and, sure enough deep in the pelvic cavity was the offending swab. She had saved the day.
Johnny Smith found his month at TQEH very worthwhile and we became good friends but, strangely, this program never took off and no further country surgeons volunteered for the program. I was the first and last.
The second interruption was by my own design. We were desperately short of furniture at home, so I volunteered my months’ annual leave to do a locum job at Woomera, allowing the incumbent, Kevin O’Grady, who had been in my year as a student, to take leave.
Again, we packed up our trusty Austin Lancer with two small children, including a cot for the younger, and set off for Woomera. In those day,s the road was unsealed and this made passing any vehicle in front impossible because of the dust thrown up. Similarly, if any vehicle passed going the other way, one had to stop and allow the dust to settle and restore visibility.
We found Woomera a godforsaken place but the work was not demanding and the money good. One interesting side benefit was that I was asked to be the doctor on site for the Eldo rocket launches and so, after returning to Adelaide, I was duly recalled to Woomera, by plane this time, and taken out to the range. Why they required a doctor on site I am not too sure as any mishap would have been monumental and too much for one doctor. I don’t think I even took a stethoscope. This was still 1967.
We had a good view from the range communications centre and excitement increased as the countdown began – fifteen seconds, fourteen, thirteen…the tension increased…then HOLD.
The blast off was postponed until the next day.
On the next day we were taken back to the range and the same thing happened – twelve seconds, eleven, ten…then again…HOLD.
This time the whole launch was abandoned and I caught the plane back to Adelaide, disappointed. It is my understanding that they never had one successful ELDO launch at Woomera, probably because each of the three stages of the rocket were designed and built by a different European nation – British, German and Italian. It was destined to be a failure!
What the ELDO blast-off should have looked like but didn’t
[1] John O’Brien, Med J Aust 1981, 1, 260-2 and online www.surgeons.org > richard-jepson-article
[2] Quoting Jim Harris, as above
[3] SA Medical Heritage Society
[4][5] As above
READ Chapter 13
